"En Física siempre hemos hecho grandes
progresos sin responder la pregunta de qué es la realidad. Solo
respondemos a la cuestión de qué se puede medir y cómo podemos observar
algo. Podemos observar la realidad, podemos hacer mediciones, pero creo
que no podemos decir nada sobre la esencia de la realidad".
“No puedes demostrar que la Luna está ahí cuando nadie mira”
Anton Zeilinger, Nobel de Física
El científico austriaco, pionero del teletransporte cuántico, reflexiona sobre Dios y la esencia de la realidad
R. Lo importante es que para demostrar que la Luna
está ahí tienes que mirarla. Si no la miras, solo puedes recurrir a tu
experiencia y a tu lógica para decir que está ahí. Pero, con las
partículas cuánticas, tú no puedes decir que el sistema está ahí si
nadie mira. Einstein preguntó: “¿De verdad crees que la Luna no está ahí
cuando nadie mira?”. Y [el físico danés Niels] Bohr respondió: “¿Puedes
demostrar lo contrario? ¿Puedes demostrar que la Luna está ahí cuando
nadie mira?”. Y no, no puedes.
P. Niels Bohr
afirmó: “Es un error pensar que la tarea de la física consiste en
averiguar cómo es la naturaleza. La física se ocupa de lo que podemos decir sobre la naturaleza”.
R.
Yo iría un paso más allá y diría: Lo que se puede decir sobre la
naturaleza, en principio, también define lo que puede existir. Así que
nada puede existir sin la posibilidad de decir algo sobre ello.
P. ¿Qué es la realidad entonces?
R.
En física siempre hemos hecho grandes progresos sin responder la
pregunta de qué es esto. Solo respondemos a la cuestión de qué se puede
medir y cómo podemos observar algo. Podemos observar la realidad,
podemos hacer mediciones, pero creo que no podemos decir nada sobre la
esencia de la realidad.
P. ¿Usted es cristiano?
R. Sí,
me crie en el catolicismo, pero mi madre era protestante, así que
aprendí de los dos. A veces iba a la iglesia protestante con mi madre y a
veces a misa católica con mi padre. Era interesante.
P. Cuando observa este mundo de partículas haciendo cosas loquísimas, ¿cómo encaja esa locura con la idea de un Dios organizado?
R. El teólogo y filósofo jesuita Karl Rahner dijo: “El cristiano del futuro será un místico
o no será”. Yo estoy de acuerdo. No se puede decir que Dios es
organizado o es así o asá. Dios no está sujeto a nuestras definiciones.
P. Quizá Dios tampoco existe sin la mirada del observador.
R. Es un tipo de observación diferente: no es con los ojos, es una observación con el alma.
Tendremos ordenadores cuánticos en el teléfono móvil dentro de 50 o 100 años
P. Tras su experimento en Canarias
afirmó que el teletransporte de información “desempeña un papel vital
en la visión de una internet cuántica global, ya que proporciona una
comunicación segura sin restricciones [...] y un aumento exponencial de
la velocidad de computación”. ¿Cuándo veremos esas promesas?
R.
Buena pregunta. Respecto a cuándo tendremos computación cuántica
completa, no lo sabemos. De hecho, hoy sería más cauto con mis
afirmaciones, porque el reto es enorme. En pequeños sistemas de
computación cuántica hay mucho trabajo en marcha, pero para los grandes
ordenadores aún queda mucho por hacer.
Anton Zeilinger fotografiado en Valencia, el 5 de junio. Mònica Torres
El sentido común es inútil en el mundo de lo extremadamente
diminuto, allí donde rigen las normas de la mecánica cuántica. Una de
las diferencias más asombrosas es que dos partículas —como dos fotones
de luz— pueden estar entrelazadas, de tal manera que lo que le ocurra a
una de ellas determinará lo que le pase a la otra, aunque estén muy
alejadas. Es lo que Einstein, escéptico, denominó “una fantasmagórica
acción a distancia”. El físico Anton Zeilinger,
nacido en la pequeña localidad austriaca de Ried im Innkreis hace 78
años, lleva un cuarto de siglo demostrando que las predicciones más
absurdas de la física cuántica son correctas. Hace poco más de una
década, su equipo logró teletransportar un estado cuántico entre dos
fotones de luz entrelazados. Uno estaba en la isla canaria de La Palma y
otro, en Tenerife. Había 143 kilómetros entre ellos.
Zeilinger, de la Universidad de Viena, ganó el Nobel de Física de 2022
por teletransportar información y allanar el camino hacia los
ordenadores cuánticos, exponencialmente más rápidos y más seguros. El
físico austriaco responde a las preguntas de EL PAÍS con un café con
leche y mirando al mar Mediterráneo, en la terraza de un hotel de
Valencia, durante una pausa en su actividad como jurado de los Premios
Rey Jaime I.
Pregunta. Usted escuchó hablar por primera vez del entrelazamiento cuántico en una conferencia en 1976. ¿Qué pensó?
Respuesta. No entendí nada. Solo comprendí que debía ser interesante.
P. ¿Cómo explica qué es el entrelazamiento a la gente sin conocimientos previos?
R. Nadie
carece por completo de conocimientos previos. El entrelazamiento de dos
partículas es como si tienes un par de dados. En un dado sale el tres y
en el otro también sale el tres. Si en un dado sale el seis, en el otro
también aparece el seis. Y siempre sale el mismo número en los dos
dados.
R.
Creo que Dios pone los números para que creamos que juega a los dados,
pero no juega a los dados. Dios dice: ahora es tres, ahora es dos, ahora
es seis. Y nosotros creemos que Dios juega a los dados.
R. Quizá lo sabe. O quizá no. Nosotros no podemos saberlo.
P. ¿Utiliza a Dios como una metáfora o cree en Dios?
R. Sí, creo. ¿Por qué no creer? El célebre Isaac Newton publicó libros sobre muchos temas, pero escribió mucho más sobre religión que sobre física. Era una persona religiosa.
Podemos observar la realidad, podemos hacer mediciones, pero no podemos decir nada sobre la esencia de la realidad
P.
Dos partículas entrelazadas se pueden imaginar como dos hermanos
gemelos que se comportan de manera similar a distancia porque comparten
el mismo ADN, pero no es así como funciona.
R. En el entrelazamiento, los dos hermanos cuánticos se comportan igual, pero sin ADN.
P. Es más que contraintuitivo. Es una locura.
R. Es una locura, sí.
P. Einstein definió el entrelazamiento como “una fantasmagórica acción a distancia”. ¿Le parece fantasmagórica?
R. Einstein utilizó la palabra alemana geisterhaft,
que significa algo así como espiritual. Es un fenómeno fantasmagórico
si pretendes explicarlo con las normas habituales. Pero en la física
cuántica sabes cómo funciona.
P. En su conferencia del Nobel proyectó una pregunta
en la pantalla: “¿Está ahí la Luna cuando nadie la mira?”. ¿Usted qué
responde?
R. Lo importante es que para demostrar
que la Luna está ahí tienes que mirarla. Si no la miras, solo puedes
recurrir a tu experiencia y a tu lógica para decir que está ahí. Pero,
con las partículas cuánticas, tú no puedes decir que el sistema está ahí
si nadie mira. Einstein preguntó: “¿De verdad crees que la Luna no está
ahí cuando nadie mira?”. Y [el físico danés Niels] Bohr respondió:
“¿Puedes demostrar lo contrario? ¿Puedes demostrar que la Luna está ahí
cuando nadie mira?”. Y no, no puedes.
P. Niels
Bohr afirmó: “Es un error pensar que la tarea de la física consiste en
averiguar cómo es la naturaleza. La física se ocupa de lo que podemos decir sobre la naturaleza”.
R.
Yo iría un paso más allá y diría: Lo que se puede decir sobre la
naturaleza, en principio, también define lo que puede existir. Así que
nada puede existir sin la posibilidad de decir algo sobre ello.
P. ¿Qué es la realidad entonces?
R.
En física siempre hemos hecho grandes progresos sin responder la
pregunta de qué es esto. Solo respondemos a la cuestión de qué se puede
medir y cómo podemos observar algo. Podemos observar la realidad,
podemos hacer mediciones, pero creo que no podemos decir nada sobre la
esencia de la realidad.
P. ¿Usted es cristiano?
R. Sí,
me crie en el catolicismo, pero mi madre era protestante, así que
aprendí de los dos. A veces iba a la iglesia protestante con mi madre y a
veces a misa católica con mi padre. Era interesante.
P. Cuando observa este mundo de partículas haciendo cosas loquísimas, ¿cómo encaja esa locura con la idea de un Dios organizado?
R. El teólogo y filósofo jesuita Karl Rahner dijo: “El cristiano del futuro será un místico
o no será”. Yo estoy de acuerdo. No se puede decir que Dios es
organizado o es así o asá. Dios no está sujeto a nuestras definiciones.
P. Quizá Dios tampoco existe sin la mirada del observador.
R. Es un tipo de observación diferente: no es con los ojos, es una observación con el alma.
Tendremos ordenadores cuánticos en el teléfono móvil dentro de 50 o 100 años
P. Tras su experimento en Canarias
afirmó que el teletransporte de información “desempeña un papel vital
en la visión de una internet cuántica global, ya que proporciona una
comunicación segura sin restricciones [...] y un aumento exponencial de
la velocidad de computación”. ¿Cuándo veremos esas promesas?
R.
Buena pregunta. Respecto a cuándo tendremos computación cuántica
completa, no lo sabemos. De hecho, hoy sería más cauto con mis
afirmaciones, porque el reto es enorme. En pequeños sistemas de
computación cuántica hay mucho trabajo en marcha, pero para los grandes
ordenadores aún queda mucho por hacer.
R.
Tienen un ordenador cuántico, pero es pequeño y solo se puede utilizar
para problemas muy especializados, no para problemas más generales. Para
tener una computadora cuántica completa necesitas unos 1.000 bits
cuánticos. Y ahora estamos hablando de sistemas con 30 o 50 bits
cuánticos.
P. Usted pronosticó en una entrevista en 2010 que en 15 o 20 años tendríamos un ordenador cuántico interesante.
R. Hoy hago el mismo pronóstico [risas]. Es imposible hablar a 20 años vista.
P. También dijo, quizá con ánimo provocativo, que en el futuro tendremos ordenadores cuánticos en el teléfono móvil.
R.
Eso será en 50 o 100 años. No lo dije para provocar, sino como desafío.
Cuando se construyeron las primeras computadoras, eran enormes,
ocupaban una habitación entera. Y entonces nadie pensaba que podías
tenerla en un teléfono móvil.
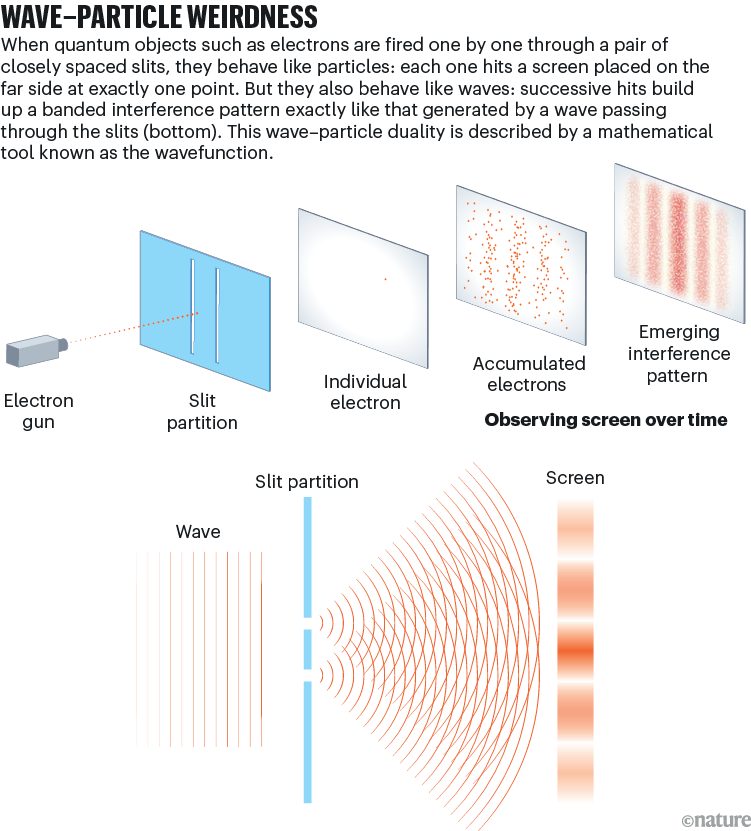
Particle, wave, both or neither? The experiment that challenges all we know about reality
Thomas Young’s double-slit experiment originally
served to prove that light is a wave — but later quantum versions have
made for a much fuzzier picture.
Thomas Young, born 250 years ago this week, was a polymath who made seminal contributions in fields from physics to Egyptology.
But perhaps his most enduring legacy is proving Isaac Newton wrong
about light — and igniting a debate about the nature of reality that
still persists.
“The experiments I am about to relate”, he told the Royal Society of London1
on 24 November 1803, “may be repeated with great ease, whenever the sun
shines.” In a simple, modern form, Young’s ‘double-slit’ experiment
involves shining light of a single frequency (say, from a red laser)
through two fine, parallel openings in an opaque sheet, onto a screen
beyond. If light were made of streams of particles, as Newton
conjectured, you would expect to see two distinct strips of light on the
screen, where the particles pile up after travelling through one slit
or the other. But that’s not what happens. Instead, you see many bands
of light and dark, strung out in stripes like a barcode: an interference
pattern (see ‘Wave–particle weirdness’).
Interference is possible only if light behaves as a wave
that strikes both slits at once and diffracts through each, creating two
sets of waves on the other side of the slits that propagate towards the
screen. Where the crest of one wave overlaps with the crest of the
other, you get constructive interference and a patch of light. Where a
crest meets a trough, you get destructive interference and darkness.
It’s
hard to overstate how wild this discovery was to physicists in Young’s
time. But the wildness truly began when Max Planck and Albert Einstein
laid the foundations for quantum mechanics in the early twentieth
century. Today, quantum mechanics forms a peerlessly accurate framework
to explain the basic elements of material reality and their
interactions. Pretty early on, it became clear that it implied that
light is made of indivisible units of energy called photons — particles,
in fact. The amount of energy each carried was proportional to the
frequency of the light. Some carry enough of a wallop to knock electrons
off atoms of metal, giving us the photoelectric effect that enables
today’s solar cells. (It was the study of this effect that led Einstein
to his conclusions about light’s particulate nature.)
With the
emergence of quantum mechanics, the idea of light as a wave faced a
challenge. But it wasn’t as simple as going back to the particle view.
Further tests of quantum theory using the double-slit experiment only
deepened the mystery. And it hasn’t been solved yet.
Singularly quantum
Imagine,
now, that your light source can shoot individual photons of red light
at the two slits, while guaranteeing that only one photon goes through
the apparatus at any time. A photographic plate on the other side
records where the photons land. Classical intuition says each photon can
go through only one slit or the other. So, this time, we should see
photons accumulating over time and forming two strips of light on the
photographic plate. Yet the mathematics of quantum theory implied that
the interference pattern would persist.
It was several decades
before the technology matured enough to verify these predictions
experimentally, using more complex set-ups that were in principle the
double-slit. At first, it wasn’t done with photons, but with electrons —
entities that we know as particles, but that quantum mechanics predicts
act as waves, too. Then, in the 1980s, a team led by Alain Aspect at
the Optical Institute in Palaiseau, France, performed the double-slit
experiment with single photons2. Quantum theory won out: an interference pattern emerged, even when only single particles passed through the slits.
Aspect won a share of the 2022 Nobel prize in physics for
his contribution to confirming the predictions of quantum mechanics
through experiment. But such experiments leave matters of interpretation
wide open. There is simply no way to comprehend what’s happening with
minds attuned to the classical world of everyday objects.
When it
comes to the double-slit experiment, quantum mechanics does tell a form
of story. It says that a photon’s position is described by a
mathematical abstraction called the wavefunction — which, as the name
suggests, behaves like a wave. This wavefunction, mathematically
speaking, hits the two slits, diffracts into two sets of waves and
recombines to create the interference pattern. The value of the
wavefunction at any location on the photographic plate lets you
calculate the probability of finding the photon there. The probability
is very high in regions of constructive interference, and very low in
regions of destructive interference.
In a sense, then, a photon or
any other quantum object acts like both a particle and a wave. This
‘wave–particle duality’ embodies many of the central conceptual
mysteries of quantum mechanics that are unresolved to this day. Even if
you could know everything about a photon’s initial state, there’s no way
to tell exactly where it’ll land on the detector. You have to talk in
terms of probabilities given by the wavefunction. These probabilities
are borne out only when thousands or tens of thousands of photons are
sent through the double slit, one by one.
Before the measurement —
in this case, detection by the photographic plate — the mathematics
says the particle exists in a superposition of states: in a sense, it
has taken both paths, through the right slit and the left. Standard
quantum mechanics says that the wavefunction ‘collapses’ when measured,
and that the act of observation in some way precipitates that collapse.
Before this, the photon has a finite probability of being found in many
different regions, but on measurement, the wavefunction peaks at the
location in which the photon appears (the probability there equals 1)
and is nullified everywhere else (probability equals 0).
It gets
even odder. If you can determine which path the photon took on its way
to the detector, it acts like a particle that does indeed go through one
slit or the other: the interference pattern disappears. But if you
cannot glean this ‘which-way’ information, the photon acts like a wave.
Whenever there are two or more ways for a photon — or, indeed, any
quantum object — to get to a final state, quantum interference occurs.
What’s a wavefunction?
But
to generate interference, something has to go through — or at least
interact in some way with — both slits. In the mathematics, the
wavefunction does the job. Some physicists would say that the
wavefunction simply represents information about the quantum system and
is not real — in which case it’s hard to explain what interacts with
both slits at once. But you can explain the interference pattern if you
consider the wavefunction to be real.
This creates its own
problems. Imagine a real wavefunction that spreads for kilometres and
kilometres before an observer detects the photon. At this point, the
wavefunction peaks at the photon’s location, and simultaneously drops to
zero everywhere else — over a large, macroscopic distance. This
suggests a kind of instantaneous, non-local influence that bothered
Einstein no end. One can avoid this with interpretations of quantum
theory that don’t collapse the wavefunction, but that opens other cans
of worms.
Thomas Young reported the results of the original double-slit experiment in the early nineteenth century.Credit: Photo Researchers/SPL
Perhaps the most notorious is the many-worlds
interpretation, the brainchild of US physicist Hugh Everett in the
1950s. This argues that every possible event — in the case of the double
slit, a particle going through the left and the right slit — happens,
each in its own world. There is no collapse: measurement simply reveals
the state of the quantum system in that world. Detractors ask how it’s
possible to justify this constant proliferation of worlds, and how, in a
many-worlds framework, you can explain why measuring quantum systems
yields probabilities, given that there are always definite outcomes in
each world.
The de Broglie–Bohm theory, named after quantum
pioneers Louis de Broglie and David Bohm, provides another alternative.
It says that particles exist with definite positions and momenta, but
are guided by an all-encompassing, invisible ‘pilot’ wave, and it’s this
wave that goes through both slits. The most profound implication of
this theory, that everything is linked to everything else in the
Universe by the underlying pilot wave, is one many physicists have
trouble accepting.
In the 1970s and 1980s, physicists upgraded the
double-slit experiment to seek clarity about the nature of quantum
reality, and the perplexing role observation apparently has in
collapsing a defined, classical reality out of it. Most notably, John
Wheeler at the University of Texas at Austin designed the ‘delayed
choice’ thought experiment3.
Imagine a double-slit set-up that gives the option of gathering or
ignoring information about which way the particle went. If you ignore
the ‘which-way’ information, you get wave-like behaviour; if you don’t,
you get particle-like patterns.
With the apparatus on the ‘collect which-way information’
setting, send a photon through the double slits. It should act like a
particle and go through one slit or the other. But just before the
photon lands on the detector, flip the apparatus to ignore the which-way
information. Will the photon, until then supposedly a particle,
suddenly switch to being a wave?
Decades later, Aspect’s team performed this experiment with single photons and showed that the answer is yes4.
Even if the photon had ostensibly travelled through the entire set-up
as a particle, switching the apparatus setting so that it ignored
which-way information caused it to act like a wave. Did the photon
travel back in time and come back through the two slits as a wave? To
avoid such nonsensical explanations, Wheeler argued that the only way to
make sense of the experiment was to say that the photon has no reality —
it’s neither wave nor particle — until it’s detected.
Back in the
1980s, Marlan Scully, then at the University of New Mexico in
Albuquerque, and his colleagues came up with a similarly befuddling
thought experiment5.
They imagined collecting the which-way information about a photon by
using a second photon ‘entangled’ with the first — a situation in which
measuring the quantum state of one tells you about the quantum state of
the other. As long as the which-way information can in principle be
extracted, the first photon should act like a particle. But if you erase
the information in the entangled partner, the mathematics showed, the
first photon goes back to behaving like a wave. In 2000, Scully, Yoon-Ho
Kim and their colleagues reported performing this experiment6. Surprisingly — or unsurprisingly, by this stage — intuition was once again defeated and quantum weirdness reigned supreme.
Larger and still larger
Others
are still pushing the double slit in new directions. This year, Romain
Tirole at Imperial College London and his colleagues described an
experiment in which the slits were temporal: one slit was open at one
point in time and the second slit an instant later7.
A beam of light that goes through these temporal slits produces an
interference pattern in its frequency spectrum. Again, the mathematics
predicts exactly this behaviour, so physicists aren’t surprised. But it
is more proof that the double-slit experiment highlights the lacunae in
our understanding of reality, a quarter of a millennium after the birth
of the man who devised it.
The double-slit experiment’s place in
the pantheon of physics experiments is assured. But it would be further
cemented if and when physicists using it were able to work out which
theory of the quantum world is correct.
For example, some theories
posit that quantum systems that grow bigger than a certain,
as-yet-undetermined size randomly collapse into classical systems, with
no observer needed. This would explain why macroscopic objects around us
don’t obviously work according to quantum rules — but how big does
something have to be before it stops acting in a quantum way?
In
2019, Markus Arndt and Yaakov Fein at the University of Vienna and their
colleagues reported sending macromolecules called oligoporphyrins,
composed of up to 2,000 atoms, through a double slit to see whether they
produce an interference pattern8.
They do, and these patterns can be explained only as a quantum
phenomenon. Arndt’s team and others continue to push such experiments to
determine whether a line exists between the quantum and the classical
world.
Last year, Siddhant Das at the Ludwig Maximilian University
of Munich, Germany, and his colleagues analysed the double-slit
experiment in the context of the de Broglie–Bohm theory9.
Unlike standard quantum mechanics, this predicts not just the
distribution of particles on the screen that leads to the spatial
interference pattern, but also the distribution of when the particles
arrive at the screen. The researchers found that their calculations on
the distribution of arrival times agreed qualitatively with observations
made two decades before, in a double-slit experiment using helium atoms10.
But it was difficult to prove their case definitively. They are
awaiting better data from a similar double-slit experiment done with
current technology, to see whether it matches predictions.
And so
it goes on, a world away from anything Young or his peers at the Royal
Society could have conceived of more than two centuries ago. “Thomas
Young would probably scratch his head if he could see the status of
today’s experiments,” says Arndt. But that’s because his experiment, so
simple in concept, has left us scratching our heads to this day.
Nature618, 454-456 (2023)
doi: https://doi.org/10.1038/d41586-023-01938-6
Updates & Corrections
Correction 20 June 2023:
An earlier version of the second picture caption gave the wrong date
for when Young reported results of a double-slit experiment.
Miller, W. A. & Wheeler, J. A. Foundations of Quantum Mechanics in the Light of New Technology (Eds Nakajima, S., Murayama, Y. & Tonomura, A.) 72–84 (World Scientific, 1997).
La erradicación de enfermedades es un
objetivo muy importante a nivel de salud pública, pero para lograrlo es
necesario implementar medidas efectivas de vigilancia, tratamiento y
control. Este hito requiere una combinación de medidas de prevención,
como la vacunación o el diagnóstico precoz, la mejora de las condiciones
sanitarias, disponer de tratamientos eficaces y contar con un músculo
fuerte en cuanto a investigación y educación.
Uno de los ejemplos más destacados es la
erradicación mundial de la viruela en 1980, lograda gracias a una
campaña masiva de vacunación. Sin embargo, la eliminación de
enfermedades es un proceso difícil y a menudo requiere una inversión
significativa en tiempo, recursos y esfuerzos.
En ese sentido, actualmente encontramos
ejemplos de enfermedades que, a pesar de disponer de tratamientos
eficaces, siguen teniendo una prevalencia relevante, como el caso de la
hepatitis C.
En nuestro país, la pandemia tuvo un
efecto devastador en términos de diagnóstico e inicio de nuevos
tratamientos respecto la hepatitis C. Según cifras de la Alianza para la
Eliminación de las Hepatitis Víricas en España (AEHVE), hay entre
20.000 y 30.000 personas que tienen la enfermedad y no lo saben. Para
conseguir el objetivo de la Organización Mundial de la Salud (OMS) de
erradicarla para el año 2030, todos los agentes del sistema deben
trabajar de forma conjunta.
Para la Dra. Marta Tejedor, jefa del Servicio de Aparato Digestivo
del Hospital Infanta Elena de Madrid, uno de los retos clave en este
sentido es “destinar más recursos a prevención primaria, insistiendo en
la educación poblacional desde temprana edad, en los colegios y
estrategias gubernamentales dirigidas a la promoción de hábitos de vida
saludables en todos los aspectos”.Según la profesional, “lo primero para
poder combatir una enfermedad es saber que existe, y si no se
visibilizan las patologías y sus consecuencias, es como si no
existieran”. Para ello, uno de los caballos de batalla más importantes
para superar este desafío es el impulso de campañas de prevención,
destaca la Dra. Tejedor.
En este sentido, la visibilización a través de estas campañas
promovería un cambio de percepción en torno a ciertas enfermedades que
conllevan un estigma asociado, como el caso de la hepatitis C. Como
comenta Tejedor, estas iniciativas ayudarían a normalizar los cribados
etarios, “igual que se hacen campañas de cáncer de colon […], la
población debe saber que la hepatitis C hoy en día se cura […] y los
tratamientos son seguros y eficaces, nada que ver con otros del pasado
como el interferón”, señala.
Por su parte, el Dr. Federico García, jefe de Servicio de
Microbiología del Hospital Universitario Clínico San Cecilio, señala que
el diagnóstico precoz y la implementación de cribados por edad son
algunos de los temas a abordar actualmente. En este sentido, subraya que
existe un debate en torno esta última cuestión, pero, desde su
experiencia, está “totalmente convencido que la edad es un factor de
riesgo para tener hepatitis C y que, por lo tanto, sería totalmente
necesario” llevar a cabo estos cribados, incide.
La
Dra. Marta Tejedor, jefa de Servicio de Aparato Digestivo del Hospital
Infanta Elena, es doctora en Medicina y especialista en Hepatología, con
un interés especial en la cirrosis avanzada y sus complicaciones. Ha
desarrollado multitud de proyectos de mejora en su servicio relacionados
con la hepatitis B, la colangitis biliar primaria y los trastornos
funcionales digestivos. Así mismo ha publicado artículos en revistas
nacionales e internacionales, ha participado en proyectos de
investigación y tiene experiencia docente con estudiantes de postgrado.
Actualmente es la coordinadora de RRSS de la Revista Española de Aparato
Digestivo, y miembro del comité ejecutivo de la Fundación Española del
Aparato Digestivo.
El éxito de las estrategias regionales
En el caso de Andalucía, una de las
regiones que ha puesto en marcha un plan estratégico para la
erradicación de la hepatitis C junto con Galicia y Cantabria, se busca
“incrementar la tasa de diagnósticos, realizar acciones en poblaciones
vulnerables y fomentar, en la medida de lo posible, cribados etarios”.
Para el Dr. García, uno de los pilares esenciales es la accesibilidad,
no en términos de acceso a tratamiento, ya que en nuestro país no
existen restricciones en ese sentido, “pero sí hay pacientes que tienen
limitaciones en el acceso al sistema sanitario”, puntualiza.
Muchos especialistas se encuentran
pacientes que son atendidos fuera del sistema, como el caso de los
centros penitenciarios o de adicciones. Por lo que, como indica
Federico, hay que “intentar mejorar y superar todas las barreras que
existen para que los pacientes tengan acceso a tratamiento, ya que,
además, en estos grupos hay una mayor prevalencia y número de casos”.
Además, incide en la importancia de contar con medidas de prevención y
de vigilancia, “necesitamos sistemas de vigilancia en tiempo real que
nos permitan conocer cifras reales de incidencia” y que ayuden a
monitorizar los potenciales casos de hepatitis C, señala García.
En este punto entran las herramientas
digitales. Ambos especialistas coinciden en la importancia de incorporar
la inteligencia artificial (IA) “a la hora de encontrar pacientes
candidatos” y “localizar a pacientes perdidos” en el sistema. En el caso
de Cantabria, por ejemplo, en Atención Primaria cuentan con un sistema
que avisa a los facultativos de que el paciente puede ser de riesgo, con
el objetivo de acelerar todo el proceso diagnóstico y contribuir a
mejorar el proceso de identificación de pacientes.
El Dr. García comenta que actualmente existen dos barreras muy
importantes en este sentido; “la propia sistemática de búsqueda”, puesto
que es un proceso muy difícil y manual. Y, en segundo lugar, la
necesidad de “elevar las tasas de rescate de los pacientes”, ya que las
tasas son bajas. Las nuevas tecnologías pueden contribuir a “conocer
cuál es la mejor estrategia para que podamos reintroducir en el sistema
sanitario todos estos pacientes que se perdieron”, afirma el
especialista.Por su parte, la Dra. Tejedor comparte la necesidad de
“automatizarlo de alguna manera”. En su opinión, contribuiría
positivamente que, si el sistema detecta algún factor de riesgo relativo
a hepatitis C, “[…] pueda pedir una analítica automáticamente para
confirmar el diagnóstico”. Sin perder el foco en que el resultado de
estas pruebas llegue a los especialistas, se dé una respuesta ágil y “el
paciente no se pierda de nuevo en el sistema”, puntualiza.
Se han dado grandes pasos en el camino hacia la erradicación de la
hepatitis C y los tratamientos antivirales han supuesto un cambio
significativo, pero todos los agentes implicados deben seguir trabajando
para mejorar el acceso al diagnóstico y aprovechar todas las
oportunidades que brindan las herramientas digitales en la lucha contra
esta enfermedad.
El
Dr. Federico García es jefe de Servicio de Microbiología del Hospital
Universitario Clínico San Cecilio. Es coordinador del área de I+D+I e
investigador Responsable del Grupo MP-13- del Instituto Biosanitario
Ibs. Granada. Asimismo, es investigador responsable de Grupo del
CIBERINFEC, vicepresidente de SEIMC e IP de diversos proyectos
nacionales y europeos. Actualmente es el director del Plan Estratégico
Andaluz para el Abordaje de las Hepatitis Virales (PEAHEP). Autor de más
de 250 publicaciones científicas, con índice H de 52.
"Cómo funciona la mente" y qué avances en neurociencia, psicología e inteligencia artificial han proporcionado nuevas perspectivas y refinado alguna de las ideas presentadas en el libro.
En el reportaje también hablo de algunas novedades editoriales como "Emocional", de@lmlodinow@Ed_Critica) o "El viaje de la humanidad", de@GalorOded(@EdDestino).
Así son los primeros compases:
"No hay nada como exponer de corrido algunas cifras sobre el cerebro humano para asimilar su vastedad, su densidad y, sobre todo, su inabarcable complejidad: apenas una masa de 1,5 kg alberga nada menos que 86 000 millones de neuronas. O dicho de otro modo, en un simple fragmento de cerebro del tamaño de un grano de arena podemos encontrar hasta 100 000 neuronas. Además, entre todas estas neuronas hay una inextricable constelación de 10 billones de sinapsis, estructuras especializadas que permiten la comunicación entre ellas. De esta manera, las neuronas se conectan entre sí o, como lo expresó el Premio Nobel Ramón y Cajal, se estrechan la mano." S.Parra
Prevalence
and clinical impact of alcohol withdrawal syndrome in
alcohol-associated hepatitis and the potential role of prophylaxis: a
multinational, retrospective cohort study
, , , , , , , , , , , , , , , , , , , , ,
a
Center
for Liver Diseases, Division of Gastroenterology, Hepatology and
Nutrition, University of Pittsburgh Medical Center, Pittsburgh, PA, USA
b
Digestive Disease Department, Clinic University Hospital, Biomedical Research Institute (INCLIVA), Valencia, Spain
c
University of California, San Francisco (UCSF), San Francisco, CA, USA
d
Department of Gastroenterology, Hospital Universitario de Canarias, Tenerife, Spain
e
Statistical Consultant Research Unit, Hospital Universitario de Canarias, Tenerife, Spain
f
Department
of Gastroenterology, Hospital Santa Creu i Sant Pau, Institut de
Recerca Sant Pau, Universidad Autónoma de Barcelona, Barcelona, Spain
g
Centro
de Investigación Biomédica en Red de Enfermedades Hepáticas y
Digestivas (CIBERehd), Instituto de Salud Carlos III, Madrid, Spain
h
Department of Pathology, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
i
Liver
Unit, Hospital Universitari Vall d'Hebron, Vall d'Hebron Institute of
Research (VHIR), Universitat Autònoma de Barcelona, Barcelona, Spain
j
Allegheny General Hospital, Pittsburgh, PA, USA
k
University of California, Davis, CA, USA
l
Liver Unit, Hospital Clinic, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain
Received
21 November 2022, Revised 29 May 2023, Accepted 31 May 2023, Available
online 22 June 2023, Version of Record 22 June 2023.
The prevalence and impact of alcohol withdrawal syndrome (AWS) in patients
with alcohol-associated hepatitis (AH) are unknown. In this study, we
aimed to investigate the prevalence, predictors, management, and
clinical impact of AWS in patients hospitalized with AH.
Methods
A multinational, retrospective cohort study
enrolling patients hospitalized with AH at 5 medical centres in Spain
and in the USA was performed between January 1st, 2016 to January 31st,
2021. Data were retrospectively retrieved from electronic health records.
Diagnosis of AWS was based on clinical criteria and use of sedatives to
control AWS symptoms. The primary outcome was mortality. Multivariable
models controlling for demographic variables and disease severity were
performed to determine predictors of AWS (adjusted odds ratio [OR]) and
the impact of AWS condition and management on clinical outcomes
(adjusted hazard ratio [HR]).
Findings
In total, 432 patients were included. The median MELD score
at admission was 21.9 (18.3–27.3). The overall prevalence of AWS was
32%. Lower platelet levels (OR = 1.61, 95% CI 1.05–2.48) and previous
history of AWS (OR = 2.09, 95% CI 1.31–3.33) were associated with a
higher rate of incident AWS, whereas the use of prophylaxis decreased
the risk (OR = 0.58, 95% CI 0.36–0.93). The use of intravenous benzodiazepines (HR = 2.18, 95% CI 1.02–4.64) and phenobarbital (HR = 2.99, 95% CI 1.07–8.37) for AWS treatment
were independently associated with a higher mortality. The development
of AWS increased the rate of infections (OR = 2.24, 95% CI 1.44–3.49),
the need for mechanical ventilation
(OR = 2.49, 95% CI 1.38–4.49), and ICU admission (OR = 1.96, 95% CI
1.19–3.23). Finally, AWS was associated with higher 28-day (HR = 2.31,
95% CI 1.40–3.82), 90-day (HR = 1.78, 95% CI 1.18–2.69), and 180-day
mortality (HR = 1.54, 95% CI 1.06–2.24).
Interpretation
AWS
commonly occurs in patients hospitalized with AH and complicates the
hospitalization course. Routine prophylaxis is associated with a lower
prevalence of AWS. Prospective studies should determine diagnostic
criteria and prophylaxis regimens for AWS management in patients with
AH.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Alcohol
withdrawal syndrome (AWS) is common in hospitalized patients with
alcohol use disorder and is associated with increased morbidity and
mortality. Recent excessive alcohol intake is key diagnostic criterion
for alcohol-associated hepatitis (AH). Thus, hospitalized patients with
AH are at high risk of developing AWS. We searched PubMed for studies
published by 1st January 2021 for articles in English using the search
term “alcohol withdrawal hepatitis” and “alcohol-associated hepatitis”.
There are no original articles evaluating the prevalence, clinical
characteristics, and management of AWS in patients with liver disease.
This fact influences that most liver societies do not recommend
homogeneous protocols to manage AWS. This is the first study evaluating
the burden, outcomes, and treatment strategies of AWS in patients
hospitalised with AH.
Added value of this study
This
is the first study evaluating AWS in patients with AH. Our findings
highlight the high burden of AWS in patients with AH. We also
demonstrated that the development of AWS is negatively associated with
increased morbidity and mortality, regardless of AH severity. Centres
that provided universal AWS prophylaxis to all patients with AH had a
lower prevalence of AWS along with overall better outcomes. Patients
with AH who developed AWS received a higher dose of benzodiazepines
(BZD) compared to previously reported in patients without AH. This is
counterintuitive as sedatives mainly have hepatic metabolism and can
cause hepatic encephalopathy, suggesting that current assessment scales
based on symptom-triggered approach need further validation in patients
with AH. The use of intravenous BZD and phenobarbital were associated
with a higher mortality rate compared to oral BZD.
Implications of all the available evidence
Our
novel findings underscore the high rate and clinical impact of AWS in
patients with AH and can serve as proof of concept for frequent
monitoring of AWS-related symptoms. Our data also should warn clinicians
on overutilization of sedatives in patients with AH as it is associated
with worse outcomes. As current AWS assessment scores are not validated
in patients with AH, we recommend favouring clinical judgment for
dosing sedatives on the basis of scaling assessment. Our findings
highlight the urgent need to conduct clinical trials to 1) assess the efficacy of AWS prophylaxis and 2) compare different AWS treatment modalities in patients with AH.
Introduction
Excessive
alcohol use is associated with a high risk of morbidity and mortality,
accounting for more than 3 million deaths per year worldwide.1,2
Over the last decade, the prevalence of alcohol use disorder (AUD) has
increased at an alarming rate with a greater rise in women, youth, and
racial minorities.3 About 50% of patients with excessive alcohol intake develop some degree of alcohol withdrawal syndrome (AWS) after abrupt cessation or reduction in alcohol intake.4 The presentation of AWS ranges from mild symptoms such as irritability, tachycardia, and tremulousness to severe forms with seizure and delirium tremens (characterized by alteration in mental status and severe autonomic hyperactivity).5 When patients with AUD are admitted into the hospital, regardless of the reason for admission, they are at risk for developing AWS. Based on a recent systematic review, among patients hospitalized for any medical condition with a history of excessive alcohol use, 2–7% develop severe AWS.6
Prolonged, heavy alcohol drinking is the most common aetiology of advanced liver disease globally.7
In parallel with the epidemic of AUD, the incidence and mortality of
alcohol-associated liver disease (ALD) are on the rise representing
about half of all liver-related mortality.2 While the majority of patients with ALD exhibit chronic hepatic changes such as steatosis or cirrhosis,
a subgroup of patients present with alcohol-associated hepatitis (AH), a
form of acute-on-chronic liver failure (ACLF) manifesting as rapid
onset of jaundice and systemic inflammation in the setting of prolonged
heavy alcohol use.8 Importantly, about 75% of patients with AH has undiagnosed cirrhosis at the time of initial presentation.9
Prolonged and heavy alcohol consumption coupled with the need for
hospitalization puts the patients AH at a high risk for the development
of AWS.
The incidence and clinical impact of AWS in patients with liver disease are unknown.10
It is plausible that early identification and appropriate management of
AWS is associated with favourable outcomes. Moreover, the safety of
current therapies has not been validated in patients with profound liver failure such as AH.11,12
Although practice guidelines for the management of AH include some
comments on management of AWS, there is little evidence to support the
use of AWS prophylaxis. Subsequently, significant variation among
different centres.13,14
While some European centres have adopted prophylactic pharmacotherapy
in patients at high risk for the development of AWS, universal
prophylaxis is highly uncommon in US centres. Furthermore, most tertiary
care centres adopt control of AWS symptoms guided by assessment scales;
however, other centres use clinical judgment for dosing of sedatives to
control AWS symptoms.15
In
this multi-national study, we aimed to describe the prevalence,
clinical characteristics, management strategies, and outcomes of AWS in
patients hospitalized with AH. We also explore the potential beneficial
effects of prophylactic therapy in patients admitted with AH by
comparing centres with different management strategies.
Methods
Study design and population
We performed a multinational, observational study identifying patients
hospitalized with AH consecutively admitted between January 1st, 2016
and January 31st, 2021. Patients from 5 tertiary medical centres were
included in this study: 4 centres from Spain (Clinic University Hospital
of Valencia, University Hospital of Canarias, Vall d’Hebron University
Hospital of Barcelona, and Santa Creu i Sant Pau Hospital of Barcelona)
and one centre from the US (University of Pittsburgh Medical Center).
All patients were aged 18 years or older at the time of hospitalization
for AH. The diagnosis of AH was based on criteria by the National
Institute on Alcohol Abuse and Alcoholism (NIAAA).13,14
Patients with histologic confirmation of AH (definite AH) and patients
with clinical characteristics of AH without any confounding findings
(probable AH) were included. Briefly, the clinical diagnostic criteria
of AH include: 1) history of alcohol use of >60 g/day in men and
>40 g/day in women, 2) an aspartate aminotransferase (AST) elevated
>1.5 times the upper limit of normal but <400 U/l with AST/ALT
ratio >1.5, 3) Serum γ-glutamyl transpeptidase (GGT) levels
>80 mg/dL, 4) altered coagulation tests [prolonged prothrombin time and/or international ratio (INR) values], and 5) serum bilirubin levels >3 mg/dL. Severe AH was defined as MELD score
>20. Exclusion criteria include 1) presence of other identifiable
causes of liver disease such as viral or autoimmune hepatitis, 2)
alternative diagnosis on liver biopsy, 3) hepatocellular carcinoma and/or other malignancies,
and 4) other extrahepatic severe illness with low life expectancy. The
study conformed to the ethical guidelines of the 1975 Declaration of
Helsinki and had the a priori approval of the institutional review
boards from all participating hospitals (2021/139, CHUC_2021_33, PR
(AG)404/2021, and STUDY 19090128). Informed consent
from patients was deemed unnecessary by the ethics committees for this
retrospective study. The study was conducted and reported in compliance
with the STROBE guidelines for cohort studies.
Data collection
Data were retrospectively retrieved from electronic health records.
Patients with a diagnosis of AH admitted to the participating centres
were consecutively enrolled. Demographic data, clinical features,
laboratory tests, management strategies, and outcomes were recorded for
every patient. Longitudinal laboratory variables were collected and used
to calculate model for end-stage liver disease (MELD),
albumin-bilirubin-INR-creatinine (ABIC), and ACLF scores at different time points of admission. The development of new organ failure during hospitalization was captured. Acute kidney injury (AKI) was defined according to the International Ascites Club. Respiratory failure was defined as SpO2/FiO2 ≤214. Cardiovascular failure was defined as mean arterial pressure less than 65 mmHg or need for vasopressors. Altered mental status was defined based on the presence of hepatic encephalopathy grade II or higher.15
Then, we calculated acute-on-chronic liver failure (ACLF) score and
categorized patients into 4 classes: no ACLF, ACLF grade I, ACLF grade
II, and ACLF grade III.16 Empirical use of antibiotic in patients with severe AH was not standard of care in any of participating centres. Use of antibiotics was based on clinician's judgement.
Data related to AWS
were captured by clinicians with experience taking care of patients
hospitalized with AH. The diagnosis of AWS was made based on the
clinical judgment of the primary clinician following the patient and the
need for sedative therapy to control AWS symptoms. Medications used for
control of AWS were categorized into benzodiazepines and phenobarbital. The route of therapy [oral versus intravenous (IV)] was recorded as well. Patients who received both oral and IV therapy were categorized in the IV group. In Spanish centres, phenobarbital is not utilized for AWS treatment. The amount of benzodiazepine was detailed in diazepam-equivalent format (https://www.benzo.org.uk/bzequiv.htm).
The duration of AWS therapy was determined by the time a patient
required medication to control AWS-related symptoms. AWS severity was
categorized into severe and non-severe based on the presence of
hallucination, delirium tremens, and/or seizures.
The severity of AWS symptoms was quantified by clinical institute
withdrawal assessment-alcohol revised (CIWA-Ar) scoring system. We also
obtained clinical complications associated with AWS, such as intubation
and ICU admission. Participating centers shared similar ICU admission
protocols and none of them considered having alcohol use disorder or AH
as a contraindication for ICU admission. Of note, the clinical protocols
for the management of AWS differed between US and Spanish centres. In
Spain, AWS prophylaxis is universally administered in all patients with a
history of recent excessive alcohol use, including all patients
admitted with AH. As a standard of care protocol, AWS prophylaxis is
given at the time of admission to all patients with AH. Prophylaxis is
largely based on clomethiazole.17 Clomethiazole is a thiamine derivative with a GABA agonist
effect commonly used for the treatment of AWS symptoms. It has been
shown clomethiazole efficacy to control AWS symptoms is not inferior to
chlordiazepoxide.18
Use of clomethiazole as a prophylaxis agent in patients at risk for AWS
is common in several European countries such as Germany or Spain.19
In the US, prophylaxis is rarely used and patients do not receive any
pharmacologic therapy until AWS symptoms start. To conduct a comparison,
cases were defined as patients diagnosed with AH by an attending
physician and requiring sedative therapy to control symptoms of AWS.8
As controls, we included all patients with AH who did not develop AWS
during the index episode. The primary outcome of the study was 28-day,
90-day, and 180-day mortality.
Statistical analysis
Qualitative
and quantitative variables were reported as absolute
frequencies/percentages and median with interquartile range (IQR),
respectively. Comparisons between groups were conducted using
Mann–Whitney U test for continuous variables and chi-square or Fisher test
for categorical variables, as appropriated. For time-to-event analysis,
the day of admission for AH was defined as the baseline point (time 0).
Censoring time was defined as the last available patient encounter,
time of death, or study closure at 180-days, whichever occurred first.
Time-to-event analysis was performed using Kaplan–Meier method. Survival
curves were compared using the log-rank test to identify parameters
modifying 28-day, 90-day, and 180-day mortality. Multivariable Cox proportional hazard regression
analyses was performed to determine the independent contribution of AWS
on mortality, adjusted for age, MELD score, ALCF class, in-hospital
infection, hepatic encephalopathy (HE), and corticosteroid use (all
considered confounding factors of AH mortality). A second model of
multivariable Cox regression was performed to determine in patients who
developed AWS the independent contribution of AWS management on
mortality, adjusted for age, MELD, HE and severity of AWS (all
considered confounding factors influencing AWS management and
mortality). The use of Cox proportional hazards models needs two
assumptions that were checked as follows: (I) Sc. Schoenfeld plot tested
that survival curves for different strata have hazard functions that
are proportional over the time t, and (II) Martingale and Schoenfeld
residuals plots tested that the relationship between the log hazard and
each covariate was linear. The results of multivariable Cox analysis are
presented as estimated hazard ratios (HR) with corresponding 95%
confidence interval (95% CI) and p-values. Collinearity was assessed
among the variables included in the multivariable analysis by using
variance inflation factors (VIF). VIFs value of less than 5 show absence
of any significant collinearity. In addition, a multivariable binary logistic regression
model adjusted for age and MELD score was performed to evaluate factors
associated with AWS (predictors and clinical outcomes). We tested
assumptions for logistic regression models that included independence of
errors, linearity in the logit for continuous variables, absence of
multicollinearity, and lack of strongly influential outliers. The
results of multivariable logistic regression are presented as estimated
odds ratio (OR) with corresponding 95% CI and p-values. All tests were
two-sided and a p-value less than 0.05 was considered statistically
significant. All analyses were performed with the IBM SPSS Statistics
for Windows, Version 25.0, Armonk, NY. The software Statistica 14.0.1.25
(tibco Software Inc.) was used to check the Cox proportional hazard
model assumptions.
Discussion
Despite
the high prevalence of AWS in AH, this is the first study investigating
the clinical characteristics, management, and outcomes of AWS in
patients hospitalized with AH. Our results revealed 6 key findings.
First, the development of AWS is common in patients hospitalized with
AH, affecting up to one-third of patients. Second, we found that
patients with AH developing AWS received high doses of BZD and
frequently through the IV route.
Third, we showed that IV BZD and phenobarbital use were associated with
worse clinical outcomes. Fourth, AWS complicated hospitalization course
by increasing the risk of in-hospital infections, need for mechanical ventilation,
and ICU admission. Fifth, we identified higher short-term and long-term
mortality in patients with AH who developed AWS. Finally, we observed a
significant disparity
in the management strategies between centres in the US and Spain.
Strikingly, AWS prophylaxis at admission in patients with AH was
associated with a lower risk of AWS development and related
complications.
In our study, up to
one-third of patients with AH developed clinically significant AWS. In a
USA cohort of patients at the Veterans Health Administration, patients
with cirrhosis had higher prevalence of AWS.12
A small study in patients with WDS undergoing a liver biopsy, found
histopathologic findings consistent with AH in 45% of patients.20
The high prevalence of AWS in patients with AH in our study is due to
the fact that most of them have a history of recent excessive alcohol
intake prior to hospitalization. In agreement with previous reports, we
showed that younger age and prior history of AWS increase the risk of
AWS in patients with AH.21
Unlike earlier reports in patients without AH, we did not find any
difference in the prevalence of AWS in AH between female and male sex.12
The high prevalence of AWS in patients with AH highlights the
importance of close monitoring in all patients admitted with AH and
strongly suggests that early prophylaxis should be instituted in order
to prevent the development and complications of AWS.
While there are no randomized controlled trials
in the management of AWS in patients with AH, we assessed various
management strategies to provide insight into the safety of current
treatment modalities and pave the way for future studies. We found that
patients with AH predominantly received a high dose of BZD and, in half
of the cases, through an IV route. When comparing our results with
previous studies in the management of AWS in patients without AH, a
higher dosage of BZD was utilized in our cohort of patients with AH.22,23
We also found the use of BZD via IV route was independently associated
with higher morbidity and mortality. BZD dosing and route of
administration are driven by a symptoms-triggered approach using
withdrawal assessment scales.23, 24, 25, 26
Higher BZD requirement in patients with AH developing AWS may be
related to overestimation of AWS severity by current scaling scores. The
lack of validity of common AWS scoring systems in face of other acute
illness were previously shown during postoperative care, leading to
inappropriately higher dose of sedative-hypnotics.27
We hypothesize that systemic inflammation related to AH may have led to
the overestimation of AWS severity, which subsequently led to higher
BZD dose and higher frequency of IV routes.28, 29, 30, 31
Validating current withdrawal severity scores in patients with AH
represents an urgent need to avoid over-utilization of BZD in patients
with AWS. Our results also warn clinicians to use the minimum dose of
BZD possible to control the symptoms and avoid IV route and
barbiturates, if possible, in patients with AH.
Poor
outcomes in patients with AH who received high dose of BZD or
phenobarbital can be related to triggering or aggravating HE, which in
turn, increase the risk of aspiration and in-hospital infection.5,32, 33, 34, 35, 36
AWS and HE have some common and distinctive symptoms and can co-exist,
making the differential diagnosis quite challenging. Currently, there is
no specific diagnostic test to reliably differentiate these two
conditions and clinician judgement (i.e., timing of symptoms onset, and
presenting symptoms) is used for this purpose, raising concern over
misdiagnosis. Although ammonia level do not guide clinical management in
HE, we showed that ammonia was slightly higher in severe AH patients
with AWS and co-existing HE.37
Furthermore, ammonia levels correlated with HE grades but not CIWA-Ar
scale. Importantly, development of HE and AWS are not mutually exclusive
and they can co-exist in about of half of patients with AH.38
It is conceivable that patients with a poor outcome after IV BZD
administration could have, at least, some degree of concomitant HE.
Prospective studies should identify novel specific diagnostic tools to
differentiate between HE and AWS. Additional causes that mimic AWS such
as Wernicke's encephalopathy should also be further investigated.
Our
findings indicate that the development of AWS is associated with a more
than two-fold risk of short-term mortality in patients admitted with
AH. The negative impact of AWS was independent of the severity of liver dysfunction,
highlighting the appropriate management of AWS as major part of AH care
to improve overall outcomes. While overall mortality of AWS in patients
admitted with alcohol intoxication is relatively low, the clinical
outcomes in patients admitted with any other indication are less
favourable.39, 40, 41
While there is no study on patients with AH, previous reports showed
that patients with advanced liver disease are at higher risk of
developing severe AWS and its related complications.42 Altered mental status resulting in a higher need for intubation and risk of aspiration pneumonia
is a potential mechanism explaining poor outcomes in patients with AH
who develop AWS. AWS can trigger alteration in mental status directly or
secondary to the use of sedatives required to control psychomotor
agitation related to AWS.
An important finding of our study is the potential beneficial role of AWS prophylaxis.43,44 Given the high burden and impact of AWS, an attempt to achieve an effective preventive strategy was pursued by few studies.45,46
However, there are no head-to-head trial comparing the outcomes of
prophylaxis with no prophylaxis in patients at risk for developing AWS.47
Based on expert opinion, AWS prophylaxis is suggested in patients at
risk for the development of severe AWS and not actively experiencing
AWS.48 Given the low level of evidence, significant variation exists among centres. A small clinical trial compared clonidinevs. diazepam as prophylaxis agents in patients at risk of AWS undergoing surgery; clonidine resulted in a lower rate of post-operative AWS.49 Clomethiazole, a fast-acting barbiturate-like drug, has been widely used for the treatment and prophylaxis of AWS in Europe.17,50 Clomethiazole was found similarly effective to BZD for treatment and prophylaxis of AWS.43,51
To the best of our knowledge, no study has evaluated the effect of
prophylaxis against AWS in patients with AH. After controlling for age
and AH severity, we found that centres adopting prophylaxis strategy had
a significantly lower rate of infection, need for mechanical
ventilation, and mortality. Results of this study strongly suggest
beneficial effects of the prophylactic regimen in all patients admitted
with AH. Further randomized controlled trials is urgently warranted to
confirm this observation.
Our study encompassed several
strengths. First, to the best of our knowledge, this is the first study
investigating the clinical characteristics, management, and outcomes of
AWS in patients with AH. Given the high prevalence of both AH and AWS,
the clinical message of this study is highly relevant to patient care.
Second, despite the multi-centre design, the study leadership was
central to ensuring universal methods for patient selection, variable
definitions, and data collection. Third, all clinical data were
collected by clinician-investigators with extensive experience in the
management of patients with AH and AWS. This should enhance the accuracy
of data by limiting the risk of inappropriate coding and documentation.
Forth, detailed clinical data on specific time-points were available
and our study contained very minimal missing data (n = 13 due to
non-reported critical laboratory values). And fifth, long-term follow up
was available in all patients, which allowed us to assess long-term
outcomes. There are, however, several limitations. First, Spanish and US
cohorts differs in several clinical aspects, severity, and management
strategies of AWS. Differences represent the heterogenous manner in
which this complication is being managed, influenced by the lack of
scientific evidence and recommendations. Although fully adjusted
multivariable analysis were performed, considering together both cohorts
can raise concern on the applicability of the results as it may be
influenced by local healthcare systems and standard of care protocols.
Nevertheless, this study allowed to compare two cohorts with different
clinical management representing a unique opportunity to assess the
potential usefulness of AWS prophylaxis and the risk of different
therapies. Our preliminary results can raise awareness of clinically
relevant issues that should now be confirmed in clinical trials.
Second, retrospective design of study incurs selection bias on
prevalence and outcomes of AWS and confounding variables. We included
patients admitted consecutively in all participating centres to minimize
this limitation. All participating centres were tertiary care hospitals
with high level of complexity, so a referral bias was likely to occur.
Thus, our results may not reflect the burden of AWS in community
centres. We attempted to control potential confounding by conducting
analysis adjusted by multiple variables and presenting the independent
measure of AWS impact on mortality and other clinical outcomes, fully
weighed with respect to critical confounders. Finally, the diagnosis of
AWS and its related complications relied on subjective judgment of
attending physician. To reduce this limitation, we confirmed their
diagnosis with the dose of as-needed sedative use and vital signs to
decrease the subjective assessments in diagnosis of AWS.
In
conclusion, this multi-center study demonstrates that AWS is common in
patients admitted with AH. AWS complicates the clinical course of
patients with AH by increasing the risk of hepatic encephalopathy,
infection, and the need for mechanical ventilation. AWS independently
increased the short-term and long-term mortality of AH. The higher dose
of sedative agents via IV route to control AWS symptoms is associated
with worse outcomes. Comparing the prophylaxis strategies between
centres, our findings suggest that adoption of universal prophylaxis
with clomethiazole may be beneficial to prevent AWS and its related
complications.