DOIhttps://doi.org/10.1007/s00431-021-04345-z
https://link.springer.com/article/10.1007/s00431-021-04345-z
-Omicron
y la incertidumbre-Agencia Sinc.es
· https://notistecnicas.blogspot.com/2021/12/omicron-y-la-incertidumbre.html
·
https://notistecnicas.blogspot.com/2021/12/hkumed-descubre-que-omicron-sars-cov-2.html
COVID-19 Año 2: Qué sabemos sobre Omicron, la variante que está
provocando millones de infecciones.
·
El Dr. JM Miró, del Hospital Clínic de Barcelona,
ofrece 45 minutos de actualización sobre Omicron, la variante del SARS-CoV-2
que está provocando millones de infecciones en todo el mundo..
·
https://www.youtube.com/watch?v=X_FuPGY5d18
·
https://www.youtube.com/channel/UCvqwrga5-pwV9Dpm8Tj7Nww
-Omicron :Resumen Grupo de Investigacion Cientifica en
Salud y tecnologia
·
Grupo de Investigacion Cientifica en Salud y tecnologia de Cochapamba,
conformado por: investigadores, médicos especialistas, medicos generales,
medicos residentes, estudiantes de medicina -Omicron ACTUALIZADO 22/12/21
· https://notistecnicas.blogspot.com/2021/12/omicron-resumen-grupo-de-investigacion.html
Transmission of SARS-CoV-2 by children
and young people in households and schools: A meta-analysis of population-based
and contact-tracing studies
· https://www.journalofinfection.com/article/S0163-4453(21)00633-2/fulltext
"Un estudio del Imperial College de
Londres concluye que la inmunidad natural generada después de la infección por
ómicron roza el 19% frente al 85% que proporcionaba Delta"
https://www.imperial.ac.uk/news/232698/omicron-largely-evades-immunity-from-past/
-Asymptomatic transmission and high
community burden of seasonal influenza in an urban and a rural community in
South Africa, 2017–18 (PHIRST): a population cohort study
https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(21)00141-8/fulltext
Early Remdesivir to Prevent Progression
to Severe Covid-19 in Outpatients
·
https://www.nejm.org/doi/full/10.1056/NEJMoa2116846?s=09
Preclinical studies demonstrate
sotrovimab retains activity against the full combination of mutations in the
spike protein of the Omicron SARS-CoV-2 variant
· https://www.gsk.com/en-gb/media/press-releases/sotrovimab-retains-activity/
SARS-CoV-2 entry sites are present in
all structural elements of the human glossopharyngeal and vagal nerves:
clinical implications
· https://www.biorxiv.org/content/10.1101/2021.12.30.474580v1
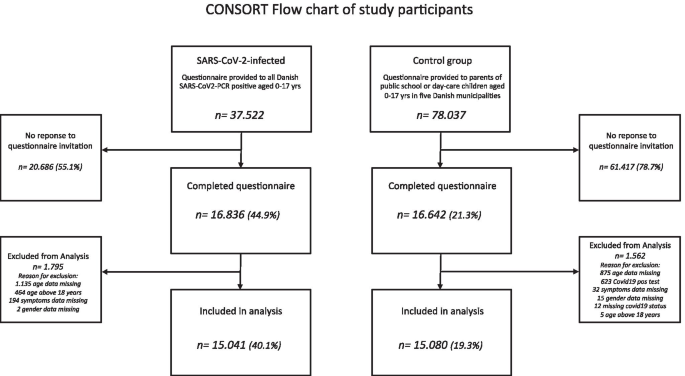
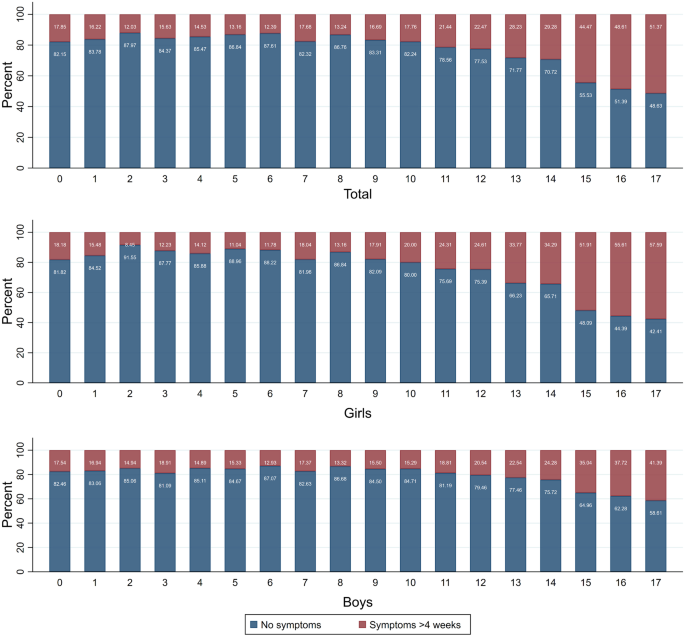
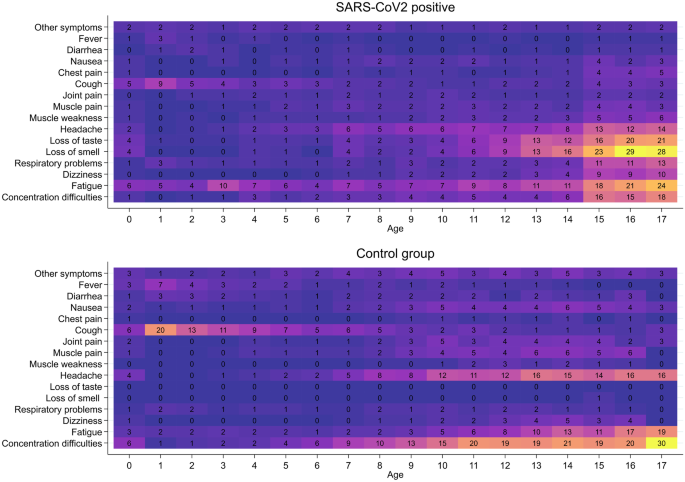
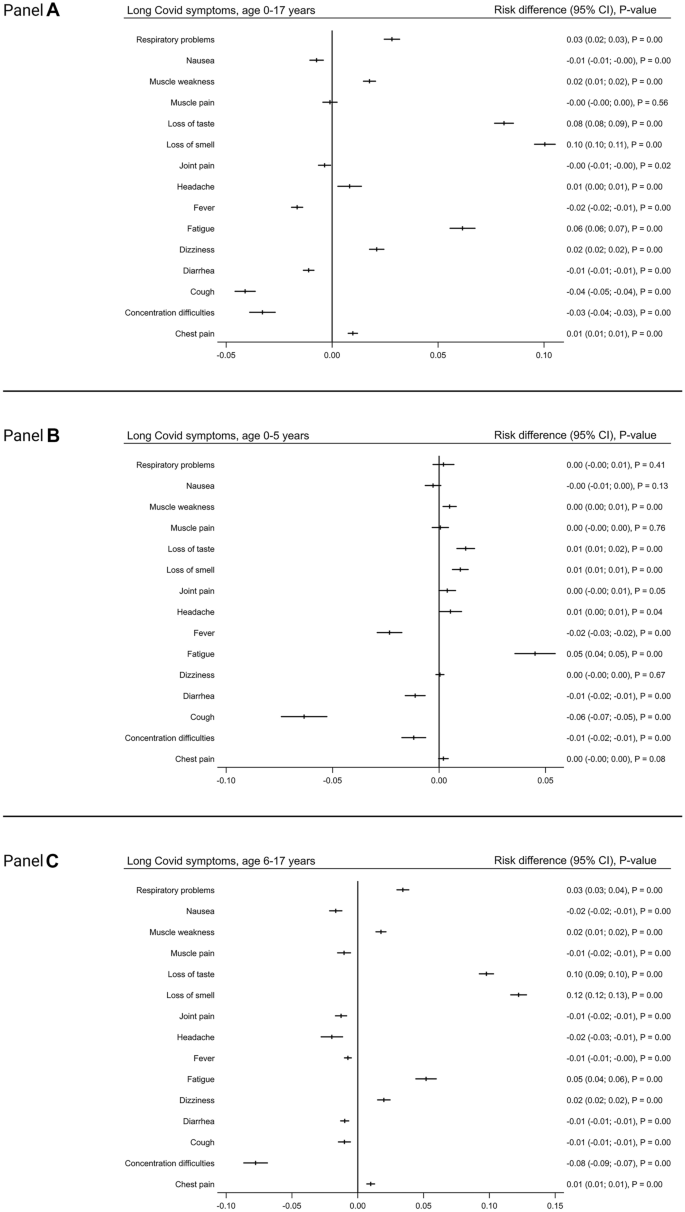
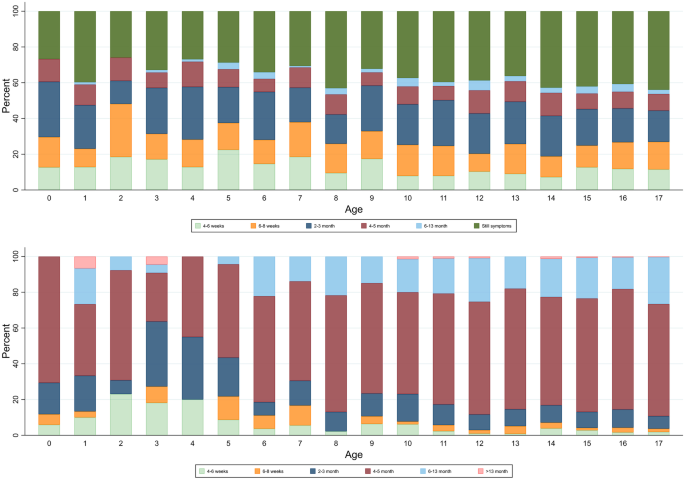
Long
COVID symptoms and duration in SARS-CoV-2 positive children — a nationwide
cohort study
https://link.springer.com/article/10.1007/s00431-021-04345-z
Vacunas
·
https://notistecnicas.blogspot.com/2021/07/el-concepto-de-eficacia-en-las-vacunas.html
Eficacia
Vacunas
·
https://articulosclaves.blogspot.com/2022/01/las-vacunas-inmunizan.html
· Vacunados/No vacunados
·
https://articulosclaves.blogspot.com/2021/12/vacunados-no-vacunados-ny-mayo.html
Vacunados versus no vacunados-Morbidity
and Mortality Weekly Report (MMWR)
https://notistecnicas.blogspot.com/2022/01/vacunados-versus-no-vacunados-morbidity.html
https://www.vozpopuli.com/espana/incidencia-hospitales-covid-gripe.html?fbclid=IwAR2dBXqpOYGeftiPGs53nf2EXfSW62VdrhJfOZ27Nqjd6Hihl4-mWMdykow
Las mutaciones del coronavirus
SARS-CoV-2
· https://notistecnicas.blogspot.com/2021/12/omicron-repaso-al-tema-mutaciones.html
https://notistecnicas.blogspot.com/2020/03/las-mutaciones-del-coronavirus-sars-cov.html
-Coronavirus: qué se sabe de las mutaciones del virus del
covid-19 (y cómo los científicos las están siguiendo en tiempo real)
·
https://www.bbc.com/mundo/noticias-52635122?fbclid=IwAR2ASsg3HFW58BKumyIRz1lCHv40ITnUVKFh0Rb1QgSjGTlpltFDpjE5TVk
-Cómo
son las mutaciones en los virus y qué sabemos en el caso del SARS-CoV-2
·
https://www.infobae.com/salud/ciencia/2021/01/09/como-son-las-mutaciones-en-los-virus-y-que-sabemos-en-el-caso-del-sars-cov-2/?fbclid=IwAR0bhu-R_0oCVPcPj5_qdzs37AXRSnetx_QhkXIoI7sKfEeW7W-H-1qMBE4
-Coronavirus: cómo mutan los virus y cómo prevén los
científicos que puede evolucionar el covid-19
· https://www.bbc.com/mundo/noticias-51835136?fbclid=IwAR2zZ47iInPB5gQyfZExpLhFIXQc2HmurWL9aUwpvPWSmKZF96Ah_QvpxTQ
Coronavirus:
qué se sabe de las mutaciones del virus del covid-19 (y cómo los científicos
las están siguiendo en tiempo real)
https://www.bbc.com/mundo/noticias-52635122?fbclid=IwAR2ASsg3HFW58BKumyIRz1lCHv40ITnUVKFh0Rb1QgSjGTlpltFDpjE5TVk
Cómo
son las mutaciones en los virus y qué sabemos en el caso del SARS-CoV-2
·
https://www.infobae.com/salud/ciencia/2021/01/09/como-son-las-mutaciones-en-los-virus-y-que-sabemos-en-el-caso-del-sars-cov-2/?fbclid=IwAR0bhu-R_0oCVPcPj5_qdzs37AXRSnetx_QhkXIoI7sKfEeW7W-H-1qMBE4
Variantes
en estudio
·
https://www.europapress.es/internacional/noticia-hallan-variante-deltacron-chipre-combinacion-variantes-delta-omicron-20220108180901.html
·
https://twitter.com/hashtag/Flurona?src=hashtag_click
·
https://twitter.com/hashtag/Deltacron?src=hashtag_click
https://articulosclaves.blogspot.com/2022/01/ba2la-llamada-variante-silenciosa-es.html
Habrá
otra variante
https://articulosclaves.blogspot.com/2022/01/habra-otra-variante-esto-es-lo-que-el.html
Estimated transmissibility and impact of
SARS-CoV-2 lineage B.1.1.7 in England
https://www.science.org/doi/10.1126/science.abg3055
La infección #Ómicron mejora la inmunidad neutralizante
contra #Delta. Esto sugiere que Ómicron
ayudará a expulsar a Delta, ya que debería disminuir la probabilidad de que
alguien infectado con Omicron se vuelva a infectar con Delta
·
https://www.niusdiario.es/ciencia-y-tecnologia/ciencia/buenas-noticias-omicron-motivos-optimismo-2022-vacunas-covid-fin-pandemia_18_3259471110.html
· https://articulosclaves.blogspot.com/2021/12/mutaciones-virus.html
· https://www.cell.com/iscience/fulltext/S2589-0042(21)01629-1?fbclid=IwAR1spjzXkY9-2wuvD-smPvUsrq0dumy1DcwfLPgdpTqycSbxVKFZFFn0RKk
https://www.niusdiario.es/ciencia-y-tecnologia/ciencia/buenas-noticias-omicron-motivos-optimismo-2022-vacunas-covid-fin-pandemia_18_3259471110.html
La infección #Ómicron mejora la
inmunidad neutralizante contra #Delta.
Esto sugiere que Ómicron ayudará a expulsar a Delta, ya que debería disminuir
la probabilidad de que alguien infectado con Omicron se vuelva a infectar con
Delta
- HKUMed descubre que Omicron SARS-CoV-2 puede infectar más
rápido y mejor que Delta en el bronquio humano pero con una infección menos
grave en el pulmón/ Evidence for a mouse origin of the SARS-CoV-2 Omicron
variant-
·
https://notistecnicas.blogspot.com/2021/12/hkumed-descubre-que-omicron-sars-cov-2.html
-
La tercera ola y el gráfico de Victor Tseng
https://notistecnicas.blogspot.com/2022/01/la-tercera-ola-y-el-grafico-de-victor.html
-Hacia el fin de la excepcionalidad
https://notistecnicas.blogspot.com/2022/01/hacia-el-fin-de-la-excepcionalidad.html
Early assessment of the clinical severity of the SARS-CoV-2 Omicron
variant in South Africa
https://www.medrxiv.org/content/10.1101/2021.12.21.21268116v1?fbclid=IwAR0HPDCG_7NOhYPVgZ9HDNOM6Eae1OgoGZLYL35snjumdoCPFF9wFxU7n5g
Severity of Omicron variant of concern
and vaccine effectiveness against symptomatic disease: national cohort with
nested test negative design study in Scotland
https://www.research.ed.ac.uk/en/publications/severity-of-omicron-variant-of-concern-and-vaccine-effectiveness-?fbclid=IwAR0paframb60xzegrAQvLfWxm-w8FYsPt6rTfdFyZdEGewJytjGFEuL7I3M
Re
Resistence of functional memory B cells
recognizing SARS-CoV-2 variants despite loss of specific IgG
·https://www.cell.com/iscience/fulltext/S2589-0042(21)01629-1?fbclid=IwAR0bhu-R_0oCVPcPj5_qdzs37AXRSnetx_QhkXIoI7sKfEeW7W-H-1qMBE4
· https://www.cell.com/iscience/fulltext/S2589-0042(21)01629-
Maduración
de la afinidad : las células B de memoria pueden modificar los Ac para
adaptarse a las modificaciones de las variantes
https://www.cell.com/iscience/fulltext/S2589-0042(21)01629-1?fbclid=IwAR1spjzXkY9-2wuvD-smPvUsrq0dumy1DcwfLPgdpTqycSbxVKFZFFn0RKk
Targeting memory T cell metabolism to improve immunity
· https://notistecnicas.blogspot.com/2021/12/t-cell-receptors-tcrs.html
https://www.jci.org/articles/view/148546?fbclid=IwAR2BMVZ2D_kKSg8Q8_ZXrf6yfZ2nXB8gmNvdWvwFXquA2rRRrVWxNETNJ-0
https://www.jci.org/review_series/117?fbclid=IwAR0FdZ7Ep_9d9R_HDNnUnkBMiEHBZg7p0fzXFLx8k-yRs1G6JbOB8JoMpus
SARS-CoV-2 spike T cell responses
induced upon vaccination or infection remain robust against Omicron
· https://notistecnicas.blogspot.com/2021/12/sars-cov-2-spike-t-cell-responses.html
Maduración
de la afinidad : las células B de memoria pueden modificar los Ac para
adaptarse a las modificaciones de las variantes
·
https://www.cell.com/iscience/fulltext/S2589-0042(21)01629-1
·
https://www.medrxiv.org/content/10.1101/2021.12.27.21268278v1.full.pdf
·
https://secureservercdn.net/50.62.198.70/1mx.c5c.myftpupload.com/wp-content/uploads/2021/12/MEDRXIV-2021-268439v1-Sigal.pdf
The omicron (B.1.1.529) SARS-CoV-2
variant of concern does not readily infect Syrian hamsters
· https://www.biorxiv.org/content/10.1101/2021.12.24.474086v1
Firma
de las células T CD8+ de memoria de larga duración en la infección aguda por
SARS-CoV-2 e Interferon
·
https://notistecnicas.blogspot.com/2021/12/firma-de-las-celulas-t-cd8-de-memoria.html
·
https://notistecnicas.blogspot.com/2021/01/asi-funcionan-las-vacunas-de-arn.html
·
https://notistecnicas.blogspot.com/2020/12/de-hungria-un-futuro-nobel-retrato-de.html
Comparison of outcomes from COVID
infection in pediatric and adult patients before and after the emergence of
Omicron
· https://www.medrxiv.org/content/10.1101/2021.12.30.21268495v1
SARS-CoV-2 and influenza virus
co-infection
· https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31052-7/fulltext#.YdIgDLgZjYM.twitter
Ómicron
infecta menos las células pulmonares
·
Al menos en modelos celulares y en hámsteres. Es verdad que no tenemos el dato
en humanos, pero
existen varios trabajos preliminares que sugieren que
la variante ómicron se multiplica peor
en células pulmonares, lo cual podría ser indicativo de su menor virulencia
(aunque habría que comprobar qué ocurre en otros órganos).
·
https://www.biorxiv.org/content/10.1101/2021.12.24.474086v1
Early assessment of the clinical
severity of the SARS-CoV-2 Omicron variant in South Africa ·
https://www.medrxiv.org/content/10.1101/2021.12.21.21268116v1?fbclid=IwAR0HPDCG_7NOhYPVgZ9HDNOM6Eae1OgoGZLYL35snjumdoCPFF9wFxU7n5g
Severity of Omicron variant of concern
and vaccine effectiveness against symptomatic disease: national cohort with
nested test negative design study in Scotland
· https://www.research.ed.ac.uk/en/publications/severity-of-omicron-variant-of-concern-and-vaccine-effectiveness-?fbclid=IwAR0paframb60xzegrAQvLfWxm-w8FYsPt6rTfdFyZdEGewJytjGFEuL7I3M
Persistence of functional memory B cells
recognizing SARS-CoV-2 variants despite loss of specific IgG
· https://www.cell.com/iscience/fulltext/S2589-0042(21)01629-1?fbclid=IwAR0bhu-R_0oCVPcPj5_qdzs37AXRSnetx_QhkXIoI7sKfEeW7W-H-1qMBE4
Maduración
de la afinidad : las células B de memoria pueden modificar los Ac para
adaptarse a las modificaciones de las variantes
·
https://www.cell.com/iscience/fulltext/S2589-0042(21)01629-1
·
https://secureservercdn.net/50.62.198.70/1mx.c5c.myftpupload.com/wp-content/uploads/2021/12/MEDRXIV-2021-268439v1-Sigal.pdf
·
El Paxlovid es un inhibidor de una de las
proteasas del SARS-CoV-2, la denominada 3CL. El tratamiento se combina con
otro inhibidor de las proteasas, el ritonavir, que ha sido empleado contra el VIH.
·
https://theconversation.com/darle-al-virus-donde-mas-le-duele-los-dos-nuevos-antivirales-contra-sars-cov-2-172461
El
anticuerpo monoclonal Sotrovimab, de la empresa GSK, también parece que es eficaz contra ómicron.
·
https://www.gsk.com/en-gb/media/press-releases/sotrovimab-retains-activity/
El
Remdesivir, un inhibidor de la ARN polimerasa viral, es otro antiviral que enpacientes
no hospitalizados con síntomas covid-19 Hasta la fecha, la actividad antiviral
de Remdesivir ha sido confirmada in vitro contra todas las otras
variantes del SARS-CoV-2, incluyendo alfa, beta, gamma, delta y épsilon.
·
https://www.nejm.org/doi/full/10.1056/NEJMoa2116846?s=09
Co-infection with SARS-CoV-2 and
Influenza A Virus in Patient with Pneumonia, China
· https://wwwnc.cdc.gov/eid/article/26/6/20-0299_article
The clinical characteristics of
pneumonia patients co-infected with 2019 novel coronavirus and influenza virus
in Wuhan, China
· https://www.researchgate.net/publication/340074430_The_clinical_characteristics_of_pneumonia_patients_co-infected_with_2019_novel_coronavirus_and_influenza_virus_in_Wuhan_China
SARS-CoV-2 and influenza virus
co-infection
· https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31052-7/fulltext
Estudio
danés sobre transmisión de Ómicron en vacunados más q en no vacunados
·
https://www.medrxiv.org/content/10.1101/2021.12.27.21268278v1
Análisis
de Rafa Toledo - JM Miro -Ignacio López-Goñi
Análisis
de Rafa Toledo
·
https://notistecnicas.blogspot.com/2021/12/omicron-repaso-al-tema-mutaciones.html
·
https://999plazaradio.valenciaplaza.com/omicron-coronavirus-vacunas-inmunizacion
·
https://notistecnicas.blogspot.com/2022/01/febrero-sera-clave-empezaran-liberarse.html
·Ómicron:
cinco buenas noticias para acabar el año Ignacio López-Goñi
·
https://theconversation.com/omicron-cinco-buenas-noticias-para-acabar-el-ano-17426
·
https://microbioblog.es/omicron-cinco-buenas-noticias-para-acabar-el-ano
·
https://www.niusdiario.es/espana/euskadi/trayecto-a-636-beasain-bergara-pago-peaje-18-enero-guipuzcoa_18_3259471342.html
·
https://articulosclaves.blogspot.com/2022/01/las-buenas-noticias-sobre-omicron-que.html
· Interferon
·
https://notistecnicas.blogspot.com/2021/06/interferon-resistance-of-emerging-sars.html
Inmunidad
·
https://notistecnicas.blogspot.com/2021/07/drosten-y-la-inmunidad-de-grupo.html
·
https://notistecnicas.blogspot.com/2021/09/inmunologia-basica-o-como-nos.html
·
https://notistecnicas.blogspot.com/2021/12/firma-de-las-celulas-t-cd8-de-memoria.html
·
https://notistecnicas.blogspot.com/2021/12/sars-cov-2-spike-t-cell-responses.html
Darle
al virus donde más le duele: los dos nuevos antivirales contra SARS-CoV-2
·
https://microbioblog.es/darle-al-virus-donde-mas-le-duele-los-dos-nuevos-antivirales-contra-sars-cov-2
·
https://notistecnicas.blogspot.com/2021/12/epidemiologia-y-dinamica-de-transmision.html
·
https://notistecnicas.blogspot.com/2022/01/enlaces-coronavirusmutaciones.html
·
https://www.eldiario.es/sociedad/ocho-meses-vacunado-puedes-no-anticuerpos-si-producirlos-celulas_128_8634187.html
·
https://notistecnicas.blogspot.com/2021/12/inmunidad-de-grupo-agutierrez.html
El
débil ataque de Omicron a los pulmones podría hacerlo menos peligroso.
Omicron’s feeble attack on the lungs
could make it less dangerous
· Mounting
evidence from animal studies suggests that Omicron does not multiply readily in
lung tissue, which can be badly damaged in people infected with other variants.
· https://www.nature.com/articles/d41586-022-00007-8
The novel coronavirus originating in
Wuhan, China: challenges for global health governance.
· View
in Article
Coronavirus disease 2019 (COVID-19)
situation report—100.
· https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200429-sitrep-100-covid-19.pdf?sfvrsn=bbfbf3d1_6
Las
vacunas inmunizan es un hecho incuestionable.
·
https://twitter.com/alfwarrior/status/1403313688623435782
·
https://twitter.com/alfwarrior/status/1476452714997506050
·
https://articulosclaves.blogspot.com/2022/01/las-vacunas-inmunizan.html
“Empezar a
reflexionar que hay que abordar la pandemia del coronavirus de una manera
diferente y pasar "de un modelo de gestión de crisis a un modelo de
control".
https://twitter.com/RanIsraeli/status/1483545718359048197
·
https://www.uppers.es/salud-bienestar/noticias-salud/gripalizar-covid-medicos-divididos-riesgos-red-centinela-sanitaria_18_3265772121.html
Viral dynamics and duration of PCR
positivity of the SARS-CoV-2 Omicron variant
https://www.medrxiv.org/content/10.1101/2022.01.13.22269257v1
https://www.medrxiv.org/content/10.1101/2022.01.10.22269010v2.full.pdf
https://www.niusdiario.es/ciencia-y-tecnologia/ciencia/cientificos-indagan-futuro-omicron-causas-mas-contagioso_18_3270496435.html
Se inicia en ensayo
clínico para analizar la eficacia y seguridad de una vacuna de Pfizer/BioNTech
diseñada específicamente contra la variante ómicron del SARS-CoV-2
https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-initiate-study-evaluate-omicron-based · ·
Llegan a España las pastillas antivirales: a quién beneficiará Paxlovid y
cómo puede ayudar a la lucha contra el Covid
https://www.elindependiente.com/vida-sana/salud/2022/01/12/llegan-a-espana-las-pastillas-antivirales-a-quien-beneficiara-paxlovid-y-como-puede-ayudar-a-la-lucha-contra-el-covid/?utm_source=share_buttons&utm_medium=twitter&utm_campaign=social_share
Gripalización
de la Pandemia
·
Tanto la Organización Mundial de la Salud (OMS) como la Agencia Europea
del Medicamento (EMA, por sus siglas en inglés), se han pronunciado estos días
sobre el error que supone empezar a tratar
la pandemia como endemia. «España quiere liderar este debate porque nos
parece necesario y oportuno abrirlo», ha sentenciado la ministra de Sanidad.
·
https://www.abc.es/sociedad/abci-coronavirus-darias-apuesta-gripalizar-covid-19-contra-criterio-y-202201121956_noticia.html
·
El único inconveniente de la ‘gripalización’ consiste en que necesita la
conformidad del virus y éste, por el momento, no se deja.
·
https://www.abc.es/opinion/abci-ignacio-camacho-gripalizar-decreto-202201120147_noticia.html
·
https://www.elplural.com/sociedad/dudas-certezas-sobre-plan-gobierno-gripalizar-coronavirus_281882102
·
https://www.elplural.com/politica/espana/sanchez-ayuso-coinciden-en-restar-gravedad-omicron_281229102
·
https://www.elplural.com/politica/sanchez-anuncia-gobierno-intervendra-precios-test-farmacias_281840102
·
Los expertos consideran que hay que cambiar la manera de abordar la
situación, pero aseguran que todavía no es el momento de gripalizar el
coronavirus.
·
https://www.antena3.com/noticias/sociedad/daniel-lopez-acuna-gripalizacion-pandemia-conveniente_2022011261de96e8192fe40001e76825.html
·
https://www.elconfidencial.com/espana/andalucia/2022-01-13/ccaa-recelan-gripalizar-covid_3358074/
Videos
·
https://www.youtube.com/watch?v=1eM1KbuNpn8
·
Desde Semergen están de acuerdo en que hay que normalizar la situación pero en
su justa medida, "sin precipitarse ni banalizar el covid diciendo que es
como la gripe porque no lo es".
·
https://www.20minutos.es/noticia/4938964/0/gripalizar-el-covid-o-coronavilizar-la-gripe-los-medicos-a-favor-y-en-contra-de-la-nueva-forma-de-seguir-la-pandemia/
·
El plan del Gobierno de la nación de pasar de fase y comenzar a ‘gripalizar’ el covid topó primero con el
rechazo de la Organización Mundial de la Salud (OMS) y después con las reticencias de las
comunidades autónomas.
·
https://www.diariodemallorca.es/nacional/2022/01/13/sanchez-detalla-gripalizacion-pandemia-sera-61541896.html
Cautelas:
Los expertos piden cautela
·
https://www.redaccionmedica.com/directo/coronavirus-ultimas-noticias/20220114
·
El presidente de SEMG de Asturias, José Miguel Álvarez Cabo, asegura que tratar
el coronavirus como gripe es precipitado y advierte de los riesgos que tendría.
·
https://www.rtpa.es/noticias-asturias-ast:--La-conveniencia-%22gripalizar%22--la-COVID-19-divide-a-los-expertos_111641900246.html
·
https://www.lavanguardia.com/vida/20220111/7978716/expertos-prematuro-gripalizar-covid.html
·
El Ministerio de Salud de Israel están sopesando un cambio de política para
alcanzar la inmunidad colectiva a través de contagios masivos con la nueva
variante.
·
https://www.epe.es/es/sanidad/20211231/medicos-idea-israel-contagio-masivo-13044572
Tasa
de incidencia-Otros baremos-Red centinela
·
¿La tasa de incidencia es siempre adecuada para
medir?
·
La media en España se sitúa en 3.042,11 por 100.000 habitantes (día 11 de enero
de 2022) https://www.elperiodico.com/es/sociedad/20220112/coronavirus-hoy-12-enero-7888927
¿Sigue
siendo el número de contagios el mejor termómetro en este punto de la pandemia?
Pablo Linde
·
https://elpais.com/sociedad/2021-07-03/sigue-siendo-el-numero-de-contagios-el-mejor-termometro-en-este-punto-de-la-pandemia.html
Estas
son las consecuencias de que, aunque se diga que no se va a hacer, sigamos basando las
expectativas en el número de contagios o la IA.
·
Rafa Toledo
·
https://twitter.com/alfwarrior/status/1473024904165535747
·
El modelo actual para decidir las medidas
restrictivas que se deben de tomar no es válido, cada comunidad ha
decidió la dureza de sus medidas con dispares resultados, en algunas
comunidades afectando gravemente a la economía de determinados sectores
Red
centinela
·
https://www.elplural.com/sociedad/dudas-certezas-sobre-plan-gobierno-gripalizar-coronavirus_281882102
Baremos
obsoletos:
·
https://www.elconfidencial.com/espana/2021-08-29/medir-riesgo-incidencia-baremos-obsoletos_3253274/
La
guerra contra Covid debería haber terminado
·
https://www.express.co.uk/comment/expresscomment/1480182/covid-war-over-no-more-lockdowns-coronavirus-comment
·
https://articulosclaves.blogspot.com/2022/01/la-guerra-contra-covid-deberia-haber.html