2019-Novel Coronavirus (2019-nCoV): estimating the case fatality rate – a word of caution
Estimating and predicting the extent and lethality of the
2019-Novel Coronavirus (2019-nCoV) outbreak, originating in Wuhan/China
is obviously challenging, reflected by many controversial statements and
reports. Unsurpassed to date, an ever-increasing flow of information,
immediately available and accessible online, has allowed the description
of this emerging epidemic in real-time [1]. The first patients were reported in Wuhan on December 31st 2019 [2].
Only a few days later, Chinese researchers identified the etiologic
agent now known as the 2019-nCoV and published the viral sequence [3].
New data on the virus, its characteristics and epidemiology become
available 24/7 and are often shared via informal platforms and media [4]. Yet, key questions remain largely unanswered.
How is the virus transmitted, how long is the incubation period,
what is the role of asymptomatic infected, what is the definite
reproductive number R0, how long is viral shedding persisting after
fading of symptoms, who is at risk for a severe course, and ultimately,
how high is the case fatality rate?
Accurate answers are critical for predicting the outbreak
dynamics, to tailor appropriate and effective prevention measures, and
to prepare for a potential pandemic. Precise estimates of the case
fatality rate and the fraction of infections that require
hospitalization are critical to balance the socioeconomic burden of
infection control interventions against their potential benefit for
mankind. Hence, one of the most important figures to determine is the
rate of asymptomatic and mild cases allowing to put severe courses and
death rates into accurate context.
At present, it is tempting to estimate the case fatality rate by
dividing the number of known deaths by the number of confirmed cases.
The resulting number, however, does not represent the true case fatality
rate and might be off by orders of magnitude. Diagnosis of viral
infection will precede recovery or death by days to weeks and the number
of deaths should therefore be compared to the past case counts –
accounting for this delay increasing the estimate of the case fatality
rate. On the other hand, cases in official statistics are likely a
severe underestimate of the total – accounting for this underestimate
will decrease the case fatality rate. The time between diagnosis and
death/recovery and the degree of underreporting will vary over time as
well as between cities and countries. A precise estimate of the case
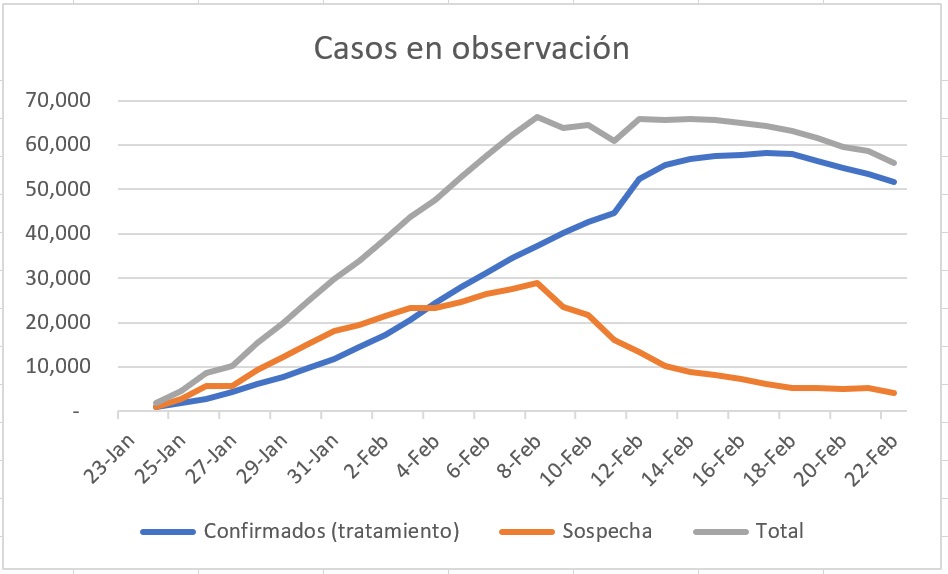
fatality rate is therefore impossible at present. Figure 1 illustrates how these uncertainties manifest themselves using currently available data.

Better estimates could be derived from large-scale
investigations, in particular, in the region of the epidemic’s origin.
Still, population-based testing of respiratory secretions by nucleic
acid amplification testing (NAT) for 2019-nCoV would most likely
underestimate the scale of the outbreak, as asymptomatic patients or
patients after recovery from infection may no longer be NAT-positive. A
sensitive 2019-nCoV-specific serological assay is needed to firmly
assess the rate of past exposure and may help to assess herd immunity.
One intriguing aspect of the outbreak so far is the discrepancy
between the estimates of the case fatality rate reported from Hubei
province, from different regions of China and from other countries. As
of February 7, 2020, 30’536 have been confirmed. Thereof, 22’112
occurred in the Hubei province of China with a death toll of 619 (=
2.8%). This contrasts with 16 deaths among 8’702 recorded cases in other
regions of China and further countries, suggesting at first glance a
case fatality rate of 0.18%. The uncertainties and spatio-temporal
variation discussed above could explain this divergence:
The higher case fatality rate reported from Wuhan may be overestimated
- The true number of exposed cases affected in Wuhan may be vastly underestimated. With a focus on thousands of serious cases, mild or asymptomatic courses that possibly account for the bulk of the 2019-nCoV infections might remain largely unrecognized, in particular during the influenza season.
- Under-detection of mild or asymptomatic cases may be further fueled after further growth of the outbreak, as healthcare-facilities and testing capacities in Wuhan have reached their limits.
Accordingly, the official numbers of both cases and deaths
reported from Wuhan represent the “tip of the iceberg”, potentially
skewing case fatality estimates towards patients presenting with more
severe disease and fatal outcome. As the current measures in Wuhan aim
at slowing the spread, other regions of China and countries gained
critical time for preparations permitting to better track cases from the
first occurrence of the virus in their populations. Thus, estimates
deriving from these settings may be more accurate. That case fatality
rates appear to decrease overall renders this hypothesis plausible.
The lower case fatality rates outside Wuhan may be underestimated
- As the epidemic arrived later in other regions and countries, there may be a delay of fatal cases arising and their reporting. The low number of documented recovered cases might indicate that days and weeks can pass until death occurs. Hence, the numbers, e.g. in Guangdong with 970 cases and no death occurring, might be false low because severe cases might still have a deadly outcome.
- Testing patients with severe respiratory diseases in outside of China might have been delayed so that unclear deaths are not yet being attributed to the coronavirus. This is unlikely at this point as international awareness has increased, but may have resulted in an underestimation of attributable deaths previously.
Case fatality rates may truly differ among different regions of the world
- Supportive care is crucial for severe respiratory disease. Differences in case fatality rates may be caused by differences in medical care during a large epidemic versus care for single cases. Hence, the large-scale capacities for medical care in the Hubei province, and specifically large-scale intensive care and extracorporeal membrane oxygenation (ECMO) may lag behind the epidemic. This hypothesis is supported by the construction of two hospitals in record time.
- There are different susceptibilities to the 2019-Novel Coronavirus in different regions of China as well as different regions of the world. However, as this is the second coronavirus emerging from China, it is unlikely that herd-immunity is lower in this region of the world, than in others. Immunogenetics and socioeconomic factors however, may potentially contribute to differences in susceptibilities to the disease.
Current authorities such as the World Health Organization, the
Centers for Disease Control & Prevention (USA), the European Centers
for Disease Control as well as renowned journals are challenged by the
rapid generation and dissemination of data, largely published on social
media platforms. Thus, new approaches will have to be defined to
validate the accuracy of such posts in times where multiple tweets per
second are published, sometimes with misleading, sometimes with
important information. Modelling the 2019-nCoV epidemic remains
challenging as relevant questions are still unanswered. So, despite the
dramatic increase of rapidly available data, public health authorities
remain torn back and forth between the options of overreacting and
frightening the population or underreacting putting citizen at risk in
their aim to provide advice to countries and individuals on measures to
protect health and prevent the spread of this outbreak.
Credits
Header image: Alissa Eckert, MS, Dan Higgins, MAM. This illustration, created at the Centers for Disease Control and Prevention (CDC), reveals ultrastructural morphology exhibited by coronaviruses. Note the spikes that adorn the outer surface of the virus, which impart the look of a corona surrounding the virion, when viewed electron microscopically. https://phil.cdc.gov/Details.aspx?pid=23312Correspondence
Prof. Manuel Battegay, MD, Division of Infectious Diseases and Hospital Epidemiology, University Hospital Basel, Petersgraben 4, CH-4031 Basel, manuel.battegay[at]usb.ch
References
1 keyboard_arrow_upLi
Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al.Early Transmission
Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N
Engl J Med. 2020;NEJMoa2001316. doi:. http://dx.doi.org/10.1056/NEJMoa2001316 PubMed
2 keyboard_arrow_upHuang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020.
3 keyboard_arrow_upWu
F, Zhao S, Yu B, Chen YM, Wang W, Song ZG, et al.A new coronavirus
associated with human respiratory disease in China. Nature. 2020. doi:. http://dx.doi.org/10.1038/s41586-020-2008-3 PubMed
4 keyboard_arrow_upWu
JT, Leung K, Leung GM. Nowcasting and forecasting the potential
domestic and international spread of the 2019-nCoV outbreak originating
in Wuhan, China: a modelling study. Lancet. 2020;S0140-6736(20)30260-9.
doi:. http://dx.doi.org/10.1016/S0140-6736(20)30260-9 PubMed
Copyright

Published under the copyright license
“Attribution – Non-Commercial – NoDerivatives 4.0”.
No commercial reuse without permission.
See: emh.ch/en/emh/rights-and-licences/
- https://smw.ch/article/doi/smw.2020.20203?fbclid=IwAR2IME8zClSEtTd_8QOuzm2ffRzuM4Anvgz-7JZ_S7QYt0XbhQHAp73M4yE
CORONAVIRUS UPDATE Febrero 23
#COVID19 #SARSCoV2
El 97,5% de
los casos confirmados siguen ocurriendo en China, el 83% en la región
del Hubei, donde además se concentra el mayor número de fallecimientos
(el 96%). El número de recuperados es ya 10 veces el de fallecimientos.

(Fuente: web)
La
enfermedad no causa síntomas o son leves en un 81% de los casos. En el
14% restante puede causar neumonía grave y en un 5% puede llegar a ser
crítica o incluso mortal. La tasa de letalidad en Hubei es del 2,3%,
fuera de esa zona puede bajar al 0,7%. Afecta principalmente a mayores
de 30 años. El 80% de los casos mortales ocurren en personas mayores de
60 años con patologías previas, más en varones que en mujeres. El
periodo de incubación medio está entre 3 y 5 días, pero se han descrito
algunos casos de más de 14 días. La transmisión es por vía aérea (por
gotículas y probablemente por aerosoles) y superficies contaminadas por
estas secreciones. Se ha detectado el virus en heces, aunque no se sabe
qué papel puede jugar esta ruta en la extensión de la enfermedad. Es muy
probable que exista transmisión del virus por personas asintomáticas,
como ocurre con otros virus de transmisión respiratoria.
China ha
aplicado unas estrictas medidas de control y cuarentena. Aunque hay que
ser precavidos, los datos actuales sugieren que de momento parece que
estas medidas están surgiendo efecto, el foco sigue centralizado en la
región de Hubei y el número de nuevos casos diarios comienzan a
disminuir.

(Fuente: @Alf_ArGzz)
Existen dos
grandes escenarios posibles: 1) que se consiga controlar al virus y
acabe desapareciendo en humanos, como pasó con el SARS del que
prácticamente no ha habido casos en los últimos quince años; 2) que el
nuevo coronavirus se incorpore a la lista de virus respiratorios como
una nueva enfermedad más o menos común. Esto último es lo que se quiere
evitar a toda costa. Un nuevo virus causante de neumonías en un 20% en
el catálogo de los patógenos respiratorios puede colapsar los sistemas
sanitarios de muchos países, aunque su letalidad sea baja. Por eso, las
medidas de cuarentena han sido tan estrictas en China.
Se han
detectado casos en 31 países, pero hay que tener en cuenta que países
donde se han notificado casos no quiere decir que el virus siga
circulando, por ejemplo España o Alemania. Hasta ahora los pocos casos
fuera de China eran sobre todo importados y muy controlados.
En los
últimos días la situación ha cambiado. Se han descrito focos en Irán,
Corea de Sur e Italia preocupantes. En Irán, 43 casos confirmados y 6
fallecimientos, proporción que hace pensar que probablemente haya muchos
más. En Corea del Sur, donde muy probablemente se confirme la
existencia de super propagadores o contagiadores, van 602 y 5
fallecimientos. Y en Italia, 155 y 3 fallecidos. De momento, en Corea e
Italia son focos localizados y limitados.
Mientras
que en China parece que los nuevo casos van disminuyendo, es muy
importante que en otros países la transmisión siga siendo localizada y
limitada y no se generalice y descontrole. La razón, como he comentado,
más que por la peligrosidad del virus es por el efecto que puede tener
en los propios sistemas sanitarios. Más grave aún sería si el virus se
extiende en países donde esos sistemas son peores que en Europa o
incluso inexistentes, como en África y partes de Latinoamérica. Estamos
en un momento de incertidumbre.
-
No hay comentarios:
Publicar un comentario