Abstract: Minimizing infections and deaths from COVID-19
are not the same thing. While society has some control on the final
number of infected individuals through intervention and mitigation
strategies, we have much greater control over the age-profile of the
final cohort of infected individuals. By ignoring this distinction,
strategies which focus on minimizing transmission rates to every extent
possible in the entire population could increase deaths among all age
groups.
We argue for what we call the heterogeneous transmission thesis:
in the response to a highly transmittable infectious disease with
highly age-variable mortality rates, death rates (for all age groups)
may be minimized by mitigation strategies which selectively
reduce transmission rates in at-risk populations, while maintaining
closer-to-normal transmission rates in low-risk populations.
Note: In our more recent preprint,
we explore the benefits of heterogeneous strategies in a model
accounting for measured interaction patterns between age groups.
http://math.cmu.edu/~wes/covid.html?fbclid=IwAR1rA1Qthi3pBZaGj3WODARfjRcMZwRjMMLXE0WELcGk418AWdhm-_V_-0c
Forecasting COVID-19 impact on hospital bed-days, ICU-days, ventilator days and deaths by US state in the next 4 months
This study presents the first set of estimates of predicted health
service utilization and deaths due to COVID-19 by day for the next 4
months for each state in the US.
Objective
To determine the extent and timing of deaths and excess demand for hospital services due to COVID-19 in the US.
Design, Setting, and Participants
This study used data on confirmed COVID-19 deaths by day from WHO
websites and local and national governments; data on hospital capacity
and utilization for US states; and observed COVID-19 utilization data
from select locations to develop a statistical model forecasting deaths
and hospital utilization against capacity by state for the US over the
next 4 months.
Results
Compared to licensed capacity and average annual occupancy rates,
excess demand from COVID-19 at the peak of the pandemic in the second
week of April is predicted to be 64,175 (95% UI 7,977 to 251,059) total
beds and 17,309 (95% UI 2,432 to 57,584) ICU beds. At the peak of the
pandemic, ventilator use is predicted to be 19,481 (95% UI 9,767 to
39,674). The date of peak excess demand by state varies from the second
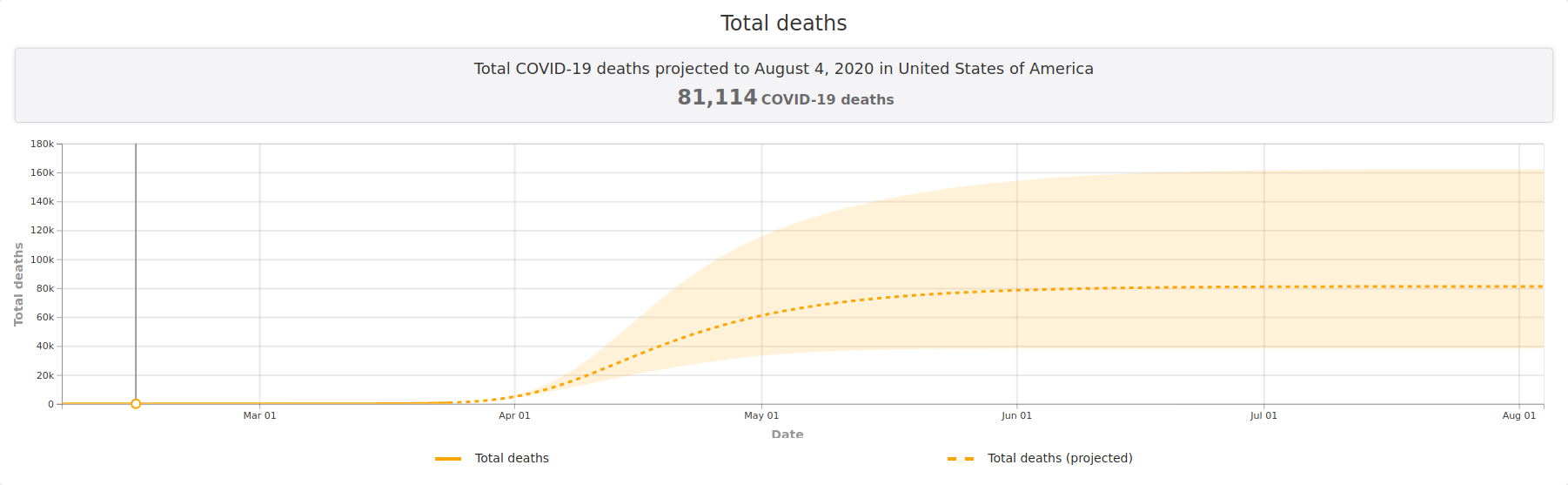
week of April through May. We estimate that there will be a total of
81,114 deaths (95% UI 38,242 to 162,106) from COVID-19 over the next 4
months in the US. Deaths from COVID-19 are estimated to drop below 10
deaths per day between May 31 and June 6.
Conclusions and Relevance
In addition to a large number of deaths from COVID-19, the epidemic
in the US will place a load well beyond the current capacity of
hospitals to manage, especially for ICU care. These estimates can help
inform the development and implementation of strategies to mitigate this
gap, including reducing non-COVID-19 demand for services and
temporarily increasing system capacity. These are urgently needed given
that peak volumes are estimated to be only three weeks away. The
estimated excess demand on hospital systems is predicated on the
enactment of social distancing measures in all states that have not done
so already within the next week and maintenance of these measures
throughout the epidemic, emphasizing the importance of implementing,
enforcing, and maintaining these measures to mitigate hospital system
overload and prevent deaths.
Citation:
IHME COVID-19 health service utilization forecasting team. Forecasting COVID-19 impact on hospital bed-days, ICU-days, ventilator days and deaths by US state in the next 4 months.MedRxiv. 26 March 2020. doi:10.1101/2020.03.27.20043752.
Recently
there has been a proliferation of modeling work which has been used to
make the point that if we can stay inside, practice extreme social
distancing, and generally lock-down nonessential parts of society for
several months, then many deaths from COVID-19 can be prevented.
For example, a new study
by Christopher J.L. Murray at the University of Washington models
hospital and ICU utilization and deaths over a 4 month period of
mitigations, and estimates that “Total deaths” can be kept under
100,000.
Murray’s study estimates hospital and ICU utilization in addition to deaths.
Like other recent studies considering short-term mitigations, he estimates fewer than 100,000 deaths.
A similar story is told by a recent model
developed by a group of researchers and publicized by Nicholas Kristof
of the New York Times. Their basic message? Social distancing for 2
months instead of 2 weeks could dramatically drop the number of COVID-19
infections:
The model publicized by Nicholas Kristof presents a dramatic benefit from 2 months of social distancing instead of 2 weeks.
The same narrative appears in recent study
in the Lancet, whose authors modeled the effects of mitigations
continuing in Wuhan through the beginning of March or the beginning of
April. In their findings, the authors write that continuing mitigations
until the beginning of April instead of the beginning of March “reduced
the median number of infections by more than 92% (IQR 66–97) and 24%
(13–90) in mid-2020 and end-2020, respectively.”.


No hay comentarios:
Publicar un comentario